
Peer Reviewed
A Rapidly Enlarging Headache
Correct Answer: D. Pott’s puffy tumor (PPT)
Treatment and management. The patient was promptly transferred to a tertiary academic pediatric hospital for treatment of presumed early PPT (Fig. 2). His physical examination redemonstrated tenderness of the frontal and maxillary sinuses and scalp swelling; extraocular movements were intact with continued photophobia. There was no nuchal rigidity and no focal neurological deficits; patient overall appeared non-toxic and active.
An MRI of the brain and orbits with and without contrast demonstrated significant purulent sinusitis, including the right frontal sinus, with possible involvement of the frontal bone and cellulitis with possible early pus pocket within the left frontal scalp but not discrete abscess. No masses or fluid collections were noted in the extra-axial spaces. Based on recommendations from the infectious disease consultant, IV vancomycin 400 mg every 8 hours (15 mg/kg) and IV ceftriaxone 1,250 mg daily (50 mg/kg) were initiated for empiric treatment on day 1 of admission. There was no evidence of epidural abscess or meningitis noted on MRI and patient was promptly treated surgically by an ear, nose, and throat (ENT) physician.
On day 2, an ENT performed right functional endoscopic sinus surgery, right maxillary antrostomy, right anterior ethmoidectomy, right frontal sinusotomy, forehead aspiration, and left nasal endoscopy; the patient tolerated the procedure well and had significant reduction of forehead and facial swelling. Sinus rinses, fluticasone propionate 50 mcg/actuation 2 intranasal sprays twice daily, and oxymetazoline 0.05% 2 intranasal sprays twice daily for 3 days were initiated following surgery. Operative cultures grew Streptococcus intermedius, thus vancomycin was discontinued on day 4 of admission, and the patient was transitioned to oral clindamycin 256.5 mg every 8 hours for 18 days and cefdinir 360 mg daily for 18 days on day 5 of admission and was discharged home on day 6 of admission in stable condition with downtrending CRP and instructed to complete a 21-day-course of these antibiotics starting from the day of surgery.
Outcome and follow-up. The patient subsequently followed up with the outpatient pediatrician 5 days after discharge with an improved condition, albeit continued headaches and photophobia. He also followed up with an infectious disease consultant the following month after completion of antibiotics, where it was noted that patient was active and playful but with occasional headaches and photophobia (optometry confirmed unaffected vision). The infectious disease consultant provided reassurance that the infection was considered successfully treated and that it would take potentially weeks for the residual forehead swelling to resolve.
Since this episode, the patient has done well overall with no recurrence of PPT. However, the patient has continued to present with sporadic episodes of sinusitis and otitis media. Fortunately, these episodes were treated successfully with amoxicillin-clavulanate without complications.
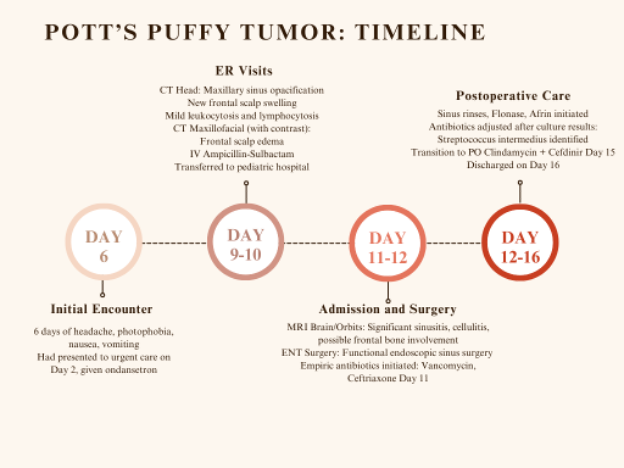
Fig. 2. A timeline of the patient’s case, which was diagnosed as Pott’s puffy tumor.
Discussion. First described by Sir Percivall Pott in 1760, PPT is a rare clinical entity characterized by subperiosteal abscess associated with osteomyelitis of the frontal bone, either directly or through hematogenous spread.1 This condition is distinct from Pott's disease associated with spinal tuberculosis, both of which were described by Sir Percival Pott.2
The differential diagnosis for this patient included new-onset migraine, acute bacterial sinusitis, orbital cellulitis, and meningitis. While migraine may present with photophobia, headache, and nausea, the imaging findings and leukocytosis are more indicative of infectious etiology rather than migraine. Acute bacterial sinusitis may present with similar symptoms, including headache, facial pain, and nasal congestion. However, PPT is distinguished by the presence of a subperiosteal abscess and frontal bone involvement, which can lead to localized swelling and potentially more severe complications, such as intracranial extension. Notably, PPT is associated with a high risk of intracranial complications in as many at 72% of cases, including epidural abscess, subdural empyema, and meningitis.3 Orbital cellulitis may also cause facial pain and swelling, especially around the eyes, but is characterized by periorbital edema and does not typically involve the frontal bone or scalp swelling seen in PPT. Lastly, meningitis presents with headache, fever, and photophobia, which overlap with the symptoms of PPT, but meningitis is typically accompanied by more systemic signs, such as neck stiffness and altered mental status, which were not observed in this patient. These differentiations underscore the importance of considering frontal bone involvement and localized swelling in the diagnosis of PPT, especially given its potential for serious intracranial complications.3
The incidence of PPT has decreased significantly due to the availability of modern antibiotics, which permit targeted therapy against causal organisms, making it a rare complication of sinusitis.3 The condition predominantly affects children and adolescents, with a mean age 11-12 years and a male-to-female ratio of approximately 7:33.4 The predilection for younger patients is likely due to the rapid development of the frontal sinuses coinciding with the peak vascularity of the affiliated valveless diploic veins.4,5 While infection may spread directly from the developing frontal sinus to the frontal bone, the draining diploic veins provide an important route for hematogenous spread, commonly leading to intracranial infection and abscess.1 Nevertheless, the exact reason for male preponderance remains unknown.6,7
As PPT is a complication of sinusitis, any condition that either disrupts the sinus anatomy or weakens the immune system increases risk. Head trauma and chronic sinusitis are import risk factors that should be gleaned from a careful history;8 likewise, presence of immunodeficiency, immunosuppression, and/or diabetes mellitus should heighten suspicion in conjunction with exam findings.9
The diagnosis of PPT involves a combination of imaging and laboratory tests. A head CT with contrast is typically the first imaging modality used due to its rapid ability to reveal key findings such as frontal sinusitis, bone erosion, and subperiosteal abscesses.8,10 Frontal sinusitis is the most frequent cause of PPT4, which was definitively noted on the second CT head with contrast. While MRI provides more detailed characterization, it may delay diagnosis due to limited availability. Laboratory tests, including CBC, ESR, and CRP, help confirm the presence and severity of infection, but may be normal in many patients.8 Early diagnosis through these methods is crucial to avoid severe complications and ensure better outcomes.3
The most common presentation of PPT includes localized, tender forehead swelling, often accompanied by sinusitis symptoms such as headache, fever, and nasal discharge. Patients may also exhibit periorbital edema or cellulitis, facial pain, and purulent or non-purulent rhinorrhea. In more severe cases, neurological symptoms, such as seizures or vision changes, may occur, underscoring the need for timely intervention.4,10 These symptoms typically evolve over a few days to weeks but may persist chronically with intermittent swelling over months.11
Generally, PPT is treated with a combination of surgical drainage and IV antibiotics. Surgical interventions are selected based on the severity and extension of infection. For infections restricted to the sinuses, an ENT surgeon may perform endoscopic sinus surgery with needle aspiration of the scalp as done in this patient. For more serious infections, such as development of epidural abscess, neurosurgical intervention is likely warranted and may include removal of affected bone.4,5,8 Concomitant culture-directed antibiotic therapy generally lasts 4 to 8 weeks, although prior reports document regimens lasting between 1 week to 7 months.4,8,10,11
The empiric antibiotic regimen for this patient included vancomycin and ceftriaxone, chosen to provide coverage against common pathogens associated with complicated sinus infections10, including Streptococcus intermedius. This organism, part of the Streptococcus anginosus group, is notable for multiple strong virulence factors and is associated with brain abscesses, rapidly progressing sinus infections, endocarditis, and pulmonary abscesses.12 Culture results confirmed Streptococcus intermedius as the causative organism, however, final culture sensitivities had not yet resulted when patient was deemed medically stable for discharge. Given patient’s excellent response to ceftriaxone, a 3rd generation cephalosporin, and lack of intracranial infection on imaging, the infectious disease consultant found it reasonable to discharge patient home on a 3-week course of cefdinir and clindamycin to target Streptococcus intermedius and other oral flora/anaerobes, respectively.
Other potentially causal organisms included Haemophilus influenzae, Moraxella catarrhalis, S. aureus, Fusobacterium, Pseudomonas, and Prevotella.11 Therefore, while initial intravenous antimicrobials should target both aerobic and anaerobic bacteria,10 antibiotic stewardship dictates narrowing coverage expediently when culture sensitivities are available.
Conclusion. When diagnosed and treated promptly, PPT generally has a favorable prognosis, with most patients recovering fully without long-term complications. However, delayed or inadequate treatment can result in severe outcomes such as brain abscesses, meningitis, or venous sinus thrombosis, which significantly increase morbidity and mortality risks. Postoperative CT sinuses of this patient taken 11 months later confirmed resolution of frontal sinus involvement, and no evidence of osteomyelitis was noted. Nevertheless, the rates of intracranial complications are high and possible recrudescence requiring repeat surgical intervention necessitates vigilance and ongoing medical follow-up.8
AUTHORS:
Justin Lien BS1 • Ananya Narasimhan BS1 • Nicholas Basalous • Evan M. Masutani MD, PhD2 • Mariam W Fahim DO1,2,3
AFFILIATIONS:
1School of Osteopathic Medicine, Western University of Health Sciences – College of Osteopathic Medicine of the Pacific, Pomona, CA
2Department of Transitional Year Residency, Southwest Healthcare Medical Education Consortium, Temecula, CA
3Inscriptions Children’s Clinic, Wildomar, CaliforniaCITATION:
Lien J, Narasimhan A, Basalous N, Masutani EM, Fahim MW. A rapidly enlarging headache. Consultant. Published online June 10, 2025. doi:10.25270/con.2025.06.000001
Received September 23, 2024. Accepted January 3, 2025.DISCLOSURES:
The authors report no relevant financial relationships.ACKNOWLEDGEMENTS:
None.CORRESPONDENCE:
Mariam W Fahim, DO, 36243 Inland Valley Dr, Wildomar, CA 92595, (mfahim@westeru.edu)
References
- Forgie SE, Marrie TJ. Pott’s puffy tumor. Am J Med. 2008;121(12):1041-1042. doi:10.1016/j.amjmed.2008.08.018
- Turgut M. Spinal tuberculosis (Pott’s disease): Its clinical presentation, surgical management, and outcome. A survey study on 694 patients. Neurosurg Rev. 2001;24(1):8-13. doi:10.1007/PL00011973
- Koltsidopoulos P, Papageorgiou E, Skoulakis C. Pott’s puffy tumor in children: A review of the literature. Laryngoscope. 2020;130(1):225-231. doi:10.1002/lary.27757
- Salomão JF, Cervante TP, Bellas AR, et al. Neurosurgical implications of Pott’s puffy tumor in children and adolescents. Childs Nerv Syst. 2014;30(9):1527-1534. doi:10.1007/s00381-014-2480-x
- Tsai BY, Lin KL, Lin TY, et al. Pott’s puffy tumor in children. Childs Nerv Syst. 2010;26(1):53-60. doi:10.1007/s00381-009-0954-z
- Clayman GL, Adams GL, Paugh DR, Koopmann CF. Intracranial complications of paranasal sinusitis: A combined institutional review. Laryngoscope. 1991;101(3):234-239. doi:10.1288/00005537-199103000-00003
- Clarós P, Ahmed H, Clarós A. Post-traumatic Pott’s puffy tumour: A case report. Eur Ann Otorhinolaryngol Head Neck Dis. 2016;133(2):119-121. doi:10.1016/j.anorl.2015.08.018
- Ketenci I, Ünlü Y, Tucer B, Vural A. The Pott’s puffy tumor: A dangerous sign for intracranial complications. Eur Arch Otorhinolaryngol. 2011;268(12):1755-1763. doi:10.1007/s00405-011-1660-5
- Paw E, Ong CT, Vangaveti V. Pott’s puffy tumour in an immunosuppressed adult: Case report and systematic review of literature. J Surg Case Rep. 2020;2020(12):1-5. doi:10.1093/jscr/rjaa528
- Daloiso A, Mondello T, Boaria F, et al. Pott’s puffy tumor in young age: A systematic review and our experience. J Clin Med. 2024;13(21):6428. doi:10.3390/jcm13216428
- Rohde RL, North LM, Murray M, Khalili S, Poetker DM. Pott’s puffy tumor: A comprehensive review of the literature. Am J Otolaryngol. 2022;43(5):103529. doi:10.1016/j.amjoto.2022.103529
- Sinha D, Sun X, Khare M, Drancourt M, Raoult D, Fournier PE. Pangenome analysis and virulence profiling of Streptococcus intermedius. BMC Genomics. 2021;22(1):1-17. doi:10.1186/s12864-021-07829-2