
HIV Management: A Practical Guide for Primary Care
With modern antiretroviral therapy (ART), human immunodeficiency virus (HIV) is a chronic, manageable condition—but outcomes hinge on rapid treatment start, durable viral suppression, and proactive primary care. Primary care clinicians can initiate and continue ART, using guideline-recommended regimens, with multidisciplinary support and specialist consultation as needed; rapid referral should not delay treatment start.1,2
HIV Diagnosis
Who to Test
The United States Preventive Services Task Force (USPSTF) currently recommends opt-out, one-time HIV screening for all individuals aged 15–65 years, with repeat testing for those at ongoing risk.3 The CDC further advises at least annual screening for higher-risk groups and notes that some, such as sexually active men who have sex with men, may benefit from screening as often as every 3–6 months. Higher-risk groups include:
- People who inject drugs and their sex partners
- People who exchange sex for money or drugs
- Sex partners of people with HIV
- Men who have sex with men
- Heterosexual patients who themselves—or whose partners—have had one or more new sex partners since the last HIV test
- People receiving treatment for hepatitis, tuberculosis, or a sexually transmitted infection (STI)
Include an HIV risk assessment at routine primary care visits for sexually active patients to determine need for more frequent screening and prevention counseling. Use a routine, opt-out approach to reduce stigma, foster earlier diagnosis and treatment, and capture patients who may not disclose risk factors; inform patients that HIV testing is part of standard preventive care and document any decision to decline. (Prevention counseling is not required for testing.) Know your state’s HIV testing laws (including reporting and partner-notification requirements) and consult CDC/state health department resources for current details.³
All sexually active adults and adolescents should be informed that pre‑exposure prophylaxis (PrEP) is available to prevent HIV acquisition. Make PrEP education and discussion a routine part of preventive care conversations, and offer or refer as indicated.3
These screening practices are intended for routine use in primary care, including wellness, prenatal, urgent-care follow-ups, and STI visits.3
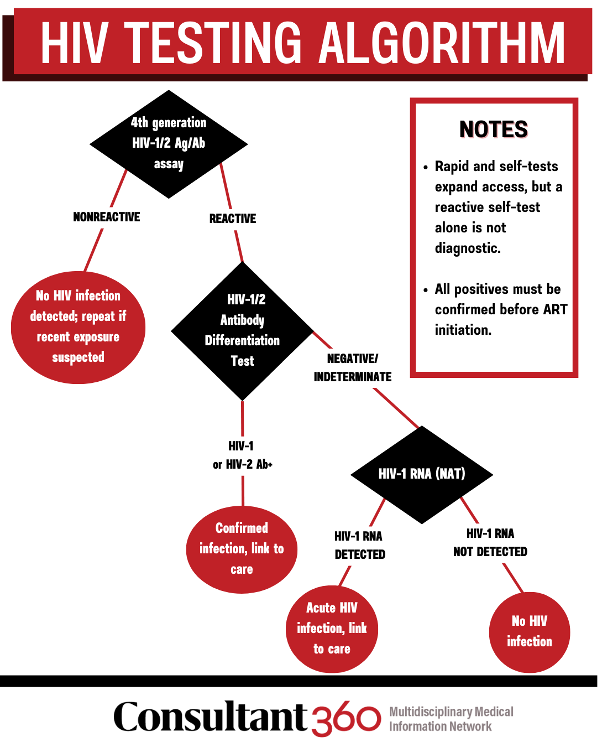
HIV Testing Algorithm
Use a laboratory-based 4th-generation HIV-1/2 Ag/Ab assay. If reactive, perform the HIV-1/2 antibody differentiation test; if negative/indeterminate with suspected acute infection, order HIV-1 RNA (NAT). Rapid and self-tests expand access, but reactive results require laboratory confirmation. A reactive self-test alone is insufficient for diagnosis; all positive results must be confirmed with a laboratory-based algorithm before antiretroviral therapy is initiated. Start linkage to care immediately after a positive result.3 This algorithm can be implemented in primary care; establish a local workflow for same-day phlebotomy and result follow-up.3
First Visit After Diagnosis: Immediate Management
Draw baseline labs but don’t delay treatment unless a specific contraindication exists. Baseline workup should include HIV RNA, CD4, resistance genotype, hepatitis B/C serologies, tuberculosis screening, pregnancy testing when relevant, and targeted metabolic/renal labs to inform regimen choice and prophylaxis.1
Begin ART at this visit unless a specific contraindication to immediate initiation exists; obtain baseline labs without delaying ART.1 Current guidelines emphasize same-day initiation of ART (“rapid start”) whenever possible, with baseline laboratory testing performed in parallel rather than delaying treatment.
Initial ART (2025 Recommendations)
First-Line Regimens
In primary care, most adults will start an integrase strand transfer inhibitor (INSTI)-based regimen—bictegravir or dolutegravir—plus two nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs), typically once daily. This is typically prescribed as a once-daily regimen. Recommended options include:
- Bictegravir/tenofovir alafenamide/emtricitabine (BIC/TAF/FTC) — single-tablet regimen containing the INSTI bictegravir and the NRTIs tenofovir alafenamide and emtricitabine.
- Dolutegravir (DTG) plus (tenofovir alafenamide/emtricitabine [TAF/FTC] or tenofovir disoproxil fumarate/emtricitabine [TDF/FTC]) — co-formulated options are commonly available; combines the INSTI dolutegravir with two NRTIs.
- Dolutegravir/lamivudine (DTG/3TC) — two-drug regimen for carefully selected patients; should be avoided in individuals with HIV RNA greater than 500,000 copies/mL, hepatitis B virus (HBV) coinfection, or when baseline resistance testing results are not yet available. Abacavir-containing regimens (eg, dolutegravir/abacavir/lamivudine) are no longer recommended for most patients because of concerns about cardiovascular risk and HLA-B*5701 hypersensitivity.
These treatment regimens are potent, well tolerated, and have high barriers to resistance.1,5
Long-Acting Injectable ART
After achieving suppression (and meeting eligibility criteria), some patients may transition to monthly or every-2-month cabotegravir/rilpivirine injections. Counsel carefully on missed-dose risks and rifamycin interactions; select patients thoughtfully.1
Consider injectables after suppression when daily pills are a barrier; coordinate administration logistics with pharmacy or multidisciplinary care partners such as nursing, and care navigators to ensure continuity of injections and adherence with dosing schedule.¹
Special Situations
In primary care, tailor initial ART in these common scenarios:¹
- HBV coinfection: Ensure the regimen covers HBV (include TAF or TDF plus FTC/3TC), or add HBV-active therapy if switching to an NRTI-sparing plan.1
- TB treatment: Rifampin induces metabolism of several ART agents; avoid long-acting cabotegravir/rilpivirine and adjust/double dolutegravir when co-administered with rifampin.1
- Pregnancy/pediatrics: Adult guidelines apply, but dosing, formulation, and safety nuances require specialist co-management; follow perinatal and pediatric HIV guidelines.1
Drug–Drug Interactions
Primary care teams should screen for drug-drug interactions (DDIs) at baseline and every visit (prescribed and over-the-counter medications, supplements).⁶ Screen DDIs before prescribing and at each visit—especially with booster-containing regimens (ritonavir/cobicistat), statins, antacids/PPIs, anticonvulsants, TB therapies, gender-affirming hormones, and long-acting injectables (which may interact for months after the last dose). Use the NIH DDI tables and a reputable checker (eg, Liverpool HIV Interactions) at point of care.6
Treatment Goals & Monitoring
Viral Suppression Targets
“Viral suppression” is generally less than 200 copies/mL; “undetectable” means below the assay’s lower limit. Multiple large studies and public health reviews have observed zero sexual transmissions when the partner with HIV maintains a documented, sustained undetectable viral load—captured in the message “Undetectable = Untransmittable” (U=U). Communicate U=U clearly: sustained viral suppression prevents sexual transmission. Reinforce U=U during visits to support adherence and reduce stigma.7-9
Monitoring Schedule
In primary care, check HIV RNA at 4–6 weeks after starting or switching ART, then every 1–3 months until suppressed; once stable and undetectable, every 3–6 months.1 CD4 can be spaced to every 6–12 months once well above opportunistic infection (OI) thresholds and virologically suppressed.1
Safety Labs & Comorbidity Checks
Reassess renal function, liver enzymes, CBC, and lipids periodically (eg, 3–6 months initially, then at least annually), tailoring to regimen and patient risk. Use single-tablet regimens or adherence supports as needed.1
Simplify to once-daily single-tablet regimens when possible, address side effects proactively, and remove barriers (transportation, pharmacy access, mental health/substance use, unstable housing). Multidisciplinary, culturally responsive models improve engagement and viral suppression.10
Opportunistic Infection Prevention
Follow the NIH, Infectious Diseases Society of America (IDSA), and HIV Medicine Association (HIVMA) opportunistic infection (OI) guidelines for primary and secondary prophylaxis, vaccination, and discontinuation criteria as CD4 T-lymphocyte counts recover on ART. Reassess OI prophylaxis at each visit; many agents can be stopped safely after immune reconstitution with sustained viral suppression
Primary prophylaxis options include:
- Pneumocystis pneumonia (PCP): Initiate prophylaxis when CD4 is less than 200 cells per microliter. The preferred agent is trimethoprim–sulfamethoxazole (TMP–SMX); consult guidelines for alternative options in patients unable to take sulfa-based medications. Discontinue prophylaxis when CD4 is greater than 200 cells per microliter for at least 3 months on effective ART.
- Toxoplasma gondii encephalitis (if immunoglobulin G [IgG] seropositive): Start prophylaxis when CD4 is less than 100 cells/µL; use the same recovery criteria to stop after immune reconstitution.
- Mycobacterium avium complex (MAC): Primary prophylaxis is not recommended for patients who initiate effective ART promptly. If ART must be delayed and CD4 is less than 50 cells/µL, consult current guideline specifics.
Re-initiate prophylaxis if CD4 again falls below the relevant thresholds.11
Comorbidity Management
Cardiovascular Risk
A 2023 randomized trial published in the New England Journal of Medicine showed pitavastatin significantly reduced major adverse cardiovascular events in people with HIV at low-to-moderate baseline risk, informing broader primary-prevention statin use in this population. Incorporate atherosclerotic cardiovascular disease risk assessment and discuss statins earlier.11 Discuss statins for primary prevention during routine primary care reviews, incorporating ASCVD risk.11,12
Metabolic Health & Weight
Some modern regimens (eg, INSTI + TAF) are associated with weight gain for a subset of patients; monitor weight and glucose, and manage cardiometabolic risk factors proactively while balancing regimen benefits. (Guideline panels discuss but do not recommend avoiding first-line INSTIs solely for weight concerns.)13 Address weight, glucose, and blood pressure using your standard primary care pathways while maintaining first-line ART when effective.1,13
Mental Health
Screen for depression, anxiety, and substance use; manage or refer mental health symptoms as needed and address adherence impacts.10
Social Determinants & Support
Address housing, food, transportation, and access barriers; leverage social work, behavioral health, and community resources. Multidisciplinary support improves engagement and viral suppression.10
Primary Care & Vaccinations in HIV
Primary care owns prevention. At routine visits, provide age-appropriate screening (diabetes, osteoporosis, cancers) and risk-based testing for STIs and hepatitis C; integrate these into chronic-care workflows for people with HIV.15
Vaccinate in primary care using ACIP’s Adult Immunization Schedule; for adults with HIV, key points include:16
- Pneumococcal: Either PCV20 or PVC21 once, or PCV15 then PPSV23 (≥8 weeks minimum interval for immunocompromised).
- Influenza: annually (inactivated or recombinant).
- Hepatitis A & B: vaccinate if nonimmune; consider CpG‑adjuvanted HepB vaccine when appropriate.
- HPV: through age 26 (consider 27–45 with shared decision-making).
- COVID-19, Tdap, zoster (RZV), meningococcal, mpox: per schedule.
- Live vaccines (MMR, varicella): generally avoid if CD4 is less than 200; may give when CD4 is 200 or greater and no contraindications. Always check the current schedule notes.16
When to Refer
Most stable patients can be managed in primary care; refer or co-manage for the following scenarios:1,10
- Persistent viremia despite adherence support
- Complex resistance history or intolerance limiting options
- Significant DDIs/polypharmacy or pregnancy planning/management
- Advanced OIs or diagnostic uncertainty
Early consultation helps maintain suppression and preserve future options.17
FAQs on HIV Management
1) How quickly should I start ART after a new diagnosis?
Immediately—ideally the same day, after drawing baseline labs. Rapid start shortens time to suppression and improves outcomes; choose a high-barrier INSTI-based regimen and adjust if resistance or HBV coinfection requires.18,19 Start same day in primary care after drawing baseline labs; do not delay for specialist scheduling.1
2) What monitoring cadence should I use once ART is started?
Check HIV RNA at 4–6 weeks, repeat every 1–3 months until suppressed, then every 3–6 months (q6 months may be reasonable after ≥2 years of stable suppression). Use less than 200 copies/mL as the clinical definition of viral suppression and reinforce U=U for patients with sustained suppression. Optimal suppression is a confirmed HIV RNA below the assay’s lower limit of detection (often <20 copies/mL).1,20
3) Which vaccines and OI prophylaxis matter most?
Give PCV20 or PCV21 (or PCV15→PPSV23), influenza annually, HepA/HepB, HPV, and others per ACIP. Avoid live vaccines if CD4 is less than 200. Start PCP prophylaxis at CD4 <200 and Toxoplasma prophylaxis at CD4 is less than 100 if IgG-positive; do not give MAC prophylaxis if ART is initiated promptly. Reassess as CD4 recovers.11,21
4) How should I manage ART in pregnancy?
Initiate ART as soon as pregnancy is recognized, regardless of trimester. Preferred regimens include dolutegravir- or raltegravir-based combinations with TDF/FTC or TAF/FTC, unless contraindicated. Continue effective ART if already on a suppressive regimen. Aim for HIV RNA suppression by delivery to minimize perinatal transmission risk. Avoid agents with known teratogenic concerns or limited pregnancy data.1
5) What are the current recommendations for long-acting ART?
Long-acting cabotegravir plus rilpivirine (LA-CAB/RPV) is an option for adults with sustained viral suppression, no resistance to either drug, and no active HBV infection. Injections are given monthly or every 2 months. It requires oral lead-in (optional but often used), strict adherence to injection schedule, and management plans for missed doses. LA regimens can improve quality of life for patients who struggle with daily oral ART but are not suitable for rapid start.17
References
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Updated September 12, 2024. Accessed August 13, 2025. https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/guidelines-adult-adolescent-arv.pdf
- World Health Organization. Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach. Geneva, Switzerland: World Health Organization; 2021. Accessed August 13, 2025. https://differentiatedservicedelivery.org/wp-content/uploads/who-consolidated-guidelines-2021.pdf
- United States Preventive Services Taskforce. Human Immunodeficiency Virus (HIV) Infection: Screening. Updated June 11,2019. Accessed August 13, 2025. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/human-immunodeficiency-virus-hiv-infection-screening
- Panel on Opportunistic Infections in Adults and Adolescents with HIV. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. Accessed August 13, 2025. https://aahivm.org/wp-content/uploads/2025/02/Guidelines-for-the-Prevention-and-Treatment-of-Opportunistic-Infections-in-Adults-and-Adolescents-With-HIV.pdf
- Gandhi RT, Landovitz RJ, Sax PE, et al. Antiretroviral drugs for treatment and prevention of HIV in adults: 2024 recommendations of the International Antiviral Society–USA panel. JAMA. 2025;333(7):609-628. doi:10.1001/jama.2024.24543
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Drug interactions overview. Accessed August 13, 2025. https://clinicalinfo.hiv-stage.od.nih.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/drug-interactions-overview
- HIV.gov. Viral suppression and an undetectable viral load. Updated February 7, 2025. Accessed August 13, 2025. https://www.hiv.gov/hiv-basics/staying-in-hiv-care/hiv-treatment/viral-suppression
- Centers for Disease Control and Prevention. Undetectable = untransmittable. Published August 19, 2024. Accessed August 13, 2025. https://www.cdc.gov/global-hiv-tb/php/our-approach/undetectable-untransmittable.html
- Huong PTT, Nguyen A, Nhan DT, Dziuban EJ, Pollack TM. The 3 moments for U=U education. Lancet HIV. 2025;12(3):e170-e172. doi:10.1016/S2352-3018(25)00013-X
- Horberg M, Thompson M, Agwu A, et al. Primary care guidance for providers of care for persons with human immunodeficiency virus: 2024 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. Published online October 12, 2024. doi:10.1093/cid/ciae479
- Spach DH. Opportunistic infections: prevention. National HIV Curriculum (University of Washington). Last updated February 3, 2025. Accessed August 13, 2025. https://www.hiv.uw.edu/pdf/co-occurring-conditions/opportunistic-infections-prevention/core-concept/all
- Grinspoon SK, Fitch KV, Zanni MV, et al. Pitavastatin to prevent cardiovascular disease in HIV infection. N Engl J Med. 2023;389(8):687-699. doi:10.1056/NEJMoa2304146
- Gandhi RT, Landovitz RJ, Sax PE, et al. Antiretroviral drugs for treatment and prevention of HIV in adults: 2024 recommendations of the International Antiviral Society–USA panel. JAMA. 2025;333(7):609-628. doi:10.1001/jama.2024.24543
- HIV Medicine Association; Infectious Diseases Society of America. Primary care guidance for persons with HIV. Guideline Central. Published October 12, 2024. Accessed August 13, 2025. https://www.guidelinecentral.com/guideline/309707/
- Thompson MA, Horberg MA, Agwu AL, et al. Primary care guidance for persons with human immunodeficiency virus: 2020 update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2021;73(11):e3572-e3605. doi:10.1093/cid/ciaa1391
- Wodi AP, Issa AN, Moser CA, Cineas S. Advisory Committee on Immunization Practices recommended immunization schedule for adults aged 19 years or older—United States, 2025. MMWR Morb Mortal Wkly Rep. 2025;74(2):30-33. doi:10.15585/mmwr.mm7402a3
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Optimizing antiretroviral therapy in the setting of virologic suppression. Accessed August 13, 2025. https://clinicalinfo.hiv-stage.od.nih.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/optimizing-antiretroviral-therapy-virologic-suppression-adult-adolescent-arv.pdf
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Initiation of antiretroviral therapy in adults and adolescents with HIV. Accessed August 13, 2025. https://clinicalinfo.hiv-stage.od.nih.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/initiation-antiretroviral-therapy-adult-adolescent-arv.pdf
- Gandhi RT, Landovitz RJ, Sax PE, et al. Antiretroviral drugs for treatment and prevention of HIV in adults: 2024 recommendations of the International Antiviral Society–USA panel. JAMA. 2025;333(7):609-628. doi:10.1001/jama.2024.24543
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Laboratory tests for initial assessment and follow-up. Accessed August 13, 2025. https://clinicalinfo.hiv-stage.od.nih.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/tests-initial-assessment-and-follow-full
- Centers for Disease Control and Prevention. Recommended immunization schedule for adults aged 19 years or older—United States, 2025. Accessed August 13, 2025. https://www.cdc.gov/vaccines/hcp/imz-schedules/downloads/adult/adult-combined-schedule.pdf
©2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Consultant360 or HMP Global, their employees, and affiliates.