
Peer Reviewed
A Rapidly Enlarging Headache
Introduction. A 6-year-old boy with a past medical history of recurrent otitis media presented to an outpatient pediatrician for subacute new-onset headache and photophobia.
History. The patient presented to the outpatient clinic for new-onset headache and photophobia, which began 6 days prior. The patient’s medical history was provided by the patient’s mother. The patient himself was unable to well-characterize the pain but noted that his headaches lasted 2-3 hours and localized to the central forehead. These headaches tended to occur in the late morning and when going to bed but did not awaken the patient from sleep and were not worse when laying down. The patient had associated nausea and vomited on the first and second day of symptoms, but no notable head trauma prior.
The patient presented to the urgent care on second day of symptoms and tested negative for SARS-COVID-19 and influenza and was sent home with ondansetron for nausea, which subsequently resolved along with the headache until the day prior (5th day of symptoms), but subsequently returned with associated ear and eye pain. He was taking alternating doses of ibuprofen and acetaminophen for headache pain relief. The patient continued to have a good appetite and denied any upper respiratory symptoms, fever, or blurry vision. There was no history of immunodeficiencies, immunosuppression, or diabetes; however, the patient had a history of recurrent ear infections. His physical examination was unremarkable and so a tentative diagnosis of new onset migraines was made, with lesser concern for increased intracranial pressure, given that headache was unaffected by posture.
The patient subsequently presented to the emergency department for headache 3 days later. His vitals were within normal limits. A non-contrast head CT was unremarkable except for asymmetric opacification of the right maxillary sinus (Figure 1A). The patient was discharged with a prescription for ondansetron and told to follow-up with the outpatient pediatrician in 1-2 days. However, the patient subsequently re-presented to the emergency department on the following day due to continued headache and new frontal scalp swelling. He was afebrile and vital signs were stable. On physical examination, the patient had tenderness to palpation of the bilateral frontal and maxillary sinuses, but no meningismus. Otoscopic examination was unremarkable. However, his laboratory tests indicated mild leukocytosis (12.36k/mcL) and mild lymphocytosis (5.3k/mcL), with SARS-COVID-19 and influenza negative. CT maxillofacial with contrast was remarkable for interval development of frontal subcutaneous scalp thickening or edema with associated frontal sinus disease (Figure 1B). There was opacification of the anterior right ethmoid air cells, right frontal ethmoidal recess, and the aerated right frontal sinus. No osteolytic or erosive changes or drainable fluid collections were noted. The patient was given 2 g of ampicillin-sulbactam IV while in the emergency department prior to transfer to a tertiary hospital.
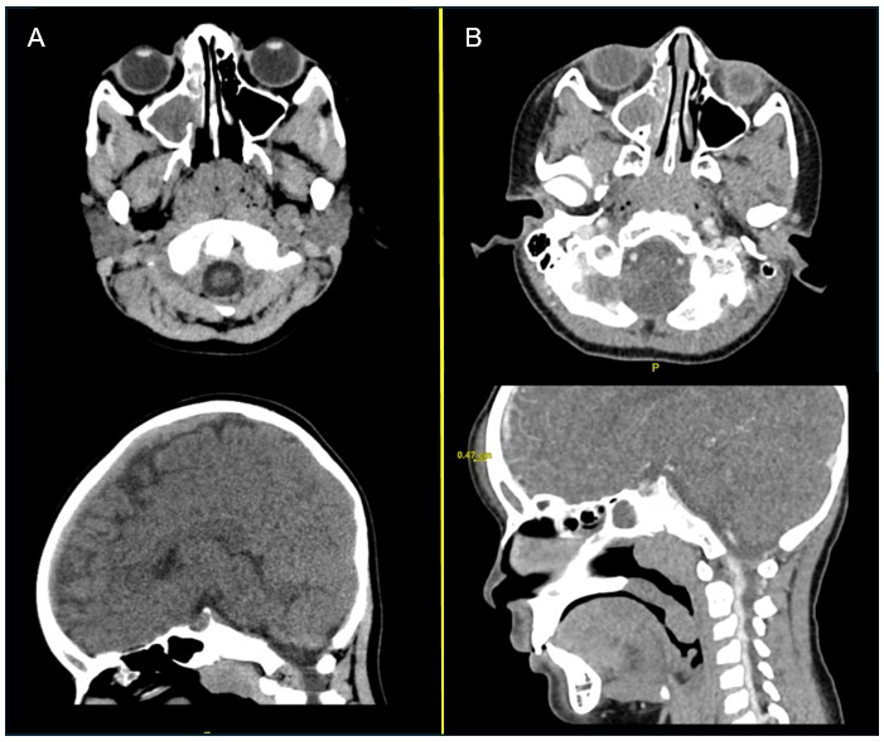
Fig. 1A-B (A) CT head non-contrast axial and coronal views during first visit to emergency department are shown. An opacification of the right maxillary sinus can be seen. (B) CT maxillofacial with contrast axial and coronal views during the second visit to the emergency department, taken 42 hours after image A is shown. Continued opacification of the right maxillary sinus and frontal sinus and interval development of frontal subcutaneous scalp thickening or edema, approximately 0.5 cm thick can be seen.