
Peer Reviewed
Odontogenic Abscess Complicated by Hyperglycemia
Authors:
Jonathan Friedman, MD
Hahnemann University Hospital/Drexel University, Philadelphia, Pennsylvania
Daniel Hsu, MS-III
Drexel University College of Medicine, Philadelphia, Pennsylvania
Robert Koenigsberg, DO
Hahnemann University Hospital/Drexel University, Philadelphia, Pennsylvania
Citation: Friedman J, Hsu D, Koenigsberg R. Odontogenic abscess complicated by hyperglycemia [published online September 28, 2018]. Infectious Diseases Consultant.
A 31-year-old man presented to the emergency department (ED) with left facial swelling and severe tooth pain. The pain had started the night of presentation, had awoken him from sleep, and was associated with headache and tinnitus.
History. The man’s medical history was significant for type 1 diabetes mellitus, hypothyroidism, and depression. He also had sustained a fractured tooth 1 year prior to presentation, at which time he had forgone treatment due to a lack of pain. At intake, his glucose level was greater than 600 mg/dL, and he stated that he had forgotten to administer his insulin lispro injection that evening.
Physical examination. The patient appeared to be in mild discomfort, with left facial swelling and a severely decayed left mandibular molar and an associated erythematous, fluctuant, 2-cm periodontal mass. His maximal interincisal opening was 30 mm, consistent with trismus, and there was palpable lymphadenopathy of the deep cervical and submandibular lymph nodes.
His vital signs included hypertension with a blood pressure of 160/89 mm Hg, heart rate of 80 beats/min, respiratory rate of 17 breaths/min, temperature of 37.2°C, and oxygen saturation of 98% on room air. His weight was 70.5 kg and his height was 178 cm, corresponding to a body mass index of 22.3 kg/m2.
Diagnostic tests. Results of a complete blood cell count, a basic metabolic panel, and blood culture tests were unremarkable aside from a glucose level of 699 mg/dL and a creatinine level of 1.21 mg/dL.
The results of contrast-enhanced maxillofacial computed tomography (CT) scans revealed an odontogenic facial soft-tissue abscess (Figures 1-3). There were partially missing first and second left mandibular molars with an adjacent rim-enhancing perimaxillary hypodensity consistent with a periapical abscess. Regional cellulitis and lymphadenopathy were present.
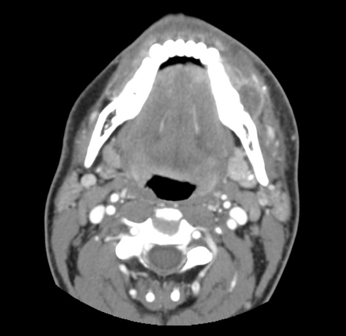
Figure 1. Axial contrast-enhanced CT showing facial swelling and cellulitis with a rim-enhancing fluid collection along the left lateral mandible.

Figure 2. Coronal contrast-enhanced CT showing the same fluid collection as it relates to an area of fractured teeth.

Figure 3. Sagittal bone window CT showing the fractured tooth responsible for the odontogenic abscess.
Management. Intravenous fluids were started, and oral narcotics were administered for pain control. Insulin was administered to control his hyperglycemia. An oral and maxillofacial surgeon was consulted for evaluation and performed an incision and drainage of the abscess. The patient was ultimately discharged from the ED with follow-up instructions.
Discussion. Odontogenic infections are a common occurrence that must be recognized and treated, since they can quickly develop into an abscess. Infections that stem from molar teeth can involve buccal, submandibular, and masticator spaces, with buccal space infections being the most prevalent.1 Buccal space involvement typically presents with cheek swelling, while submandibular space involvement generally can elicit trismus and swelling of the submandibular triangle.2
Persons who are especially susceptible to odontogenic infection and abscess formation include those with poor dental hygiene and those lacking proper dental care. Persons who lack a sufficient immune response are also particularly at risk, such as those with HIV or, as in our patient’s case, diabetes mellitus.
Odontogenic abscesses are primarily treated with surgical drainage, which is generally complemented with broad-spectrum antibiotics. Indications for the use of antibiotics include the presence of trismus, fever, cellulitis, lymphadenopathy, swelling beyond the alveolar process, and osteomyelitis.3 Penicillin or clindamycin (if a patient is allergic to penicillin) plus metronidazole for anaerobes usually constitute adequate coverage, but in immunocompromised patients, methicillin-resistant Staphylococcus aureus (MRSA) must be taken into account, as well.4,5 It is also important to support the patient medically and treat the underlying risk factors (such as controlling hyperglycemia).
The culprits of these abscesses often are polymicrobial, originating from the normal oral flora; in one study, 50% of odontogenic infections were caused by purely anaerobic bacteria, while only 6% were caused by purely aerobic flora. The remaining 44% comprised mixed aerobic and anaerobic bacteria.6 In another study, viridans streptococci were the most common aerobe, while Prevotella species comprised the majority of anaerobes.7 The source of infection, such as the tooth itself, should also be extracted.
Odontogenic abscesses require prompt treatment due to possible late advanced complications, especially when the infection spreads to fascial spaces and beyond. Due to the anatomical location and its proximity to other deep spaces such as retropharyngeal space or danger space, the abscess in fascial spaces can lead to airway compromise, causing stridor, hoarseness, or respiratory distress. When the infection spreads hematogenously beyond the cervical spaces, cavernous sinus thrombosis, sepsis, mediastinitis, or even endocarditis are among the potential complications.8 Patients with oral trauma or diabetes are especially vulnerable to deep cervical space infections.9 With MRSA infections, uncommon complications such as osteomyelitis also must be taken into consideration. In cases where mandibular molars are involved but have gone untreated, Ludwig angina is also a potential serious consequence of infection. Ludwig angina is characterized by rapidly spreading cellulitis, bilateral swelling of the mandibles, drooling, and airway obstruction.10
Predictors of prognosis include the extent and location of the infection and abscess, along with complications and antibiotic sensitivities of the pathogens. Patients with diabetes and severe infections have been shown to have a longer length of hospital stay.9 Immunocompromised patients are also at higher risk for potential complications.
- Santosh AN, Viresh AN, Sharmada BK. Microbiology and antibiotic sensitivity of odontogenic space infection. Int J Med Dent Sci. 2014;3(1):303-313.
- Ogle OE. Odontogenic Infections. Dent Clin North Am. 2017;61(2):235-25
- Flynn TR. Principles of management and prevention of odontogenic infections. In: Hupp JR, Ellis E III, Tucker MR, eds. Contemporary Oral and Maxillofacial Surgery. 6th ed. St Louis, MO: Elsevier Mosby; 2014:296-318.
- Chemaly D. How do I manage a patient with an extensive odontogenic infection? J Can Dent Assoc. 2014;80:e15.
- Cooper MN, Abrishamian LK, Newton KI. Odontogenic abscess. J Emerg Med. 2013;45(1):86-87.
- Brook I, Frazier EH, Gher ME. Aerobic and anaerobic microbiology of periapical abscess. Oral Microbiol Immunol. 1991;6(2):123-125.
- Warnke PH, Becker ST, Springer ING, et al. Penicillin compared with other advanced broad spectrum antibiotics regarding antibacterial activity against oral pathogens isolated from odontogenic abscesses. J Craniomaxillofac Surg. 2008;36(8):462-46
- Opitz D, Camerer C, Camerer D-M, et al. Incidence and management of severe odontogenic infections—a retrospective analysis from 2004 to 2011. J Craniomaxillofac Surg. 2015;43(2):285-289.
- Flynn TR, Shanti RM, Hayes C. Severe odontogenic infections, part 2: prospective outcomes study. J Oral Maxillofac Surg. 2006;64(7):1104-1113.
- Ferrera PC, Busino LJ, Snyder HS. Uncommon complications of odontogenic infections. Am J Emerg Med. 1996;14(3):317-322.