
Peer Reviewed
Progressive Oral Pigmentation in a Young Woman
Introduction. A 19-year-old collegiate athlete presented with progressive darkening of the lips and oral mucosa beginning in the summer of 2022 (Figure 1A-B). The pigmentation, which began on her lips, extended over time to her tongue, buccal mucosa, and gingiva. She reported feeling well and was otherwise in good health.
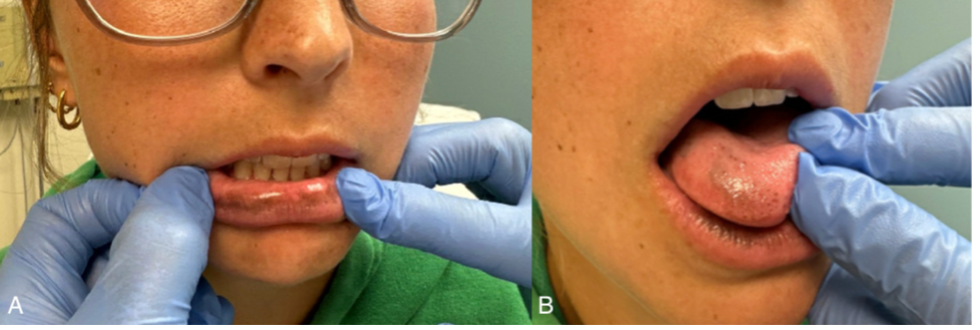
Figure 1A-B. The patient presents with hyperpigmented macules on the lips, tongue, buccal mucosa, and gingiva.History. The patient had no significant past medical history and no relevant family history of autoimmune disorders, aside from maternal hypothyroidism. She denied using medications commonly associated with drug-induced pigmentation, such as minocycline or doxycycline.1 She had recently started taking oral contraceptives around the time of symptom onset. Her initial physical examination confirmed hyperpigmented macules of the lips, tongue, buccal mucosa, and gingiva, as well as linear pigmentation in 1 thumbnail and toenail changes consistent with trauma.
Over the following year, the patient developed systemic symptoms, including fatigue, salt craving, dizziness on standing, decreased appetite, and unintentional weight loss. By the age of 20, the patient’s pigmentation had progressed alongside increasing systemic symptoms. Her physical examination 9 months later now revealed hyperpigmented freckles and scars in addition to oral mucosal changes (Figure 2).

Figure 2. Hyperpigmentation of the lips, tongue, buccal mucosa, and gingiva with hyperpigmented freckles and scars can be seen at 9 months following her initial presentation.Diagnostic and laboratory testing. Laboratory tests revealed a significantly elevated adrenocorticotropic hormone (ACTH) level (>2000 pg/mL, [normal range, ~7-63 pg/mL]) and a low morning cortisol concentration (3.3 μg/dL, [normal range at 6am-8am, ~10-20 mcg/dL]). Patch testing yielded negative results. Although biopsy and histopathological analyses may have provided additional insight, they were deemed unnecessary given the laboratory findings and accompanying systemic symptomatology.