
Peer Reviewed
Hyperpigmented Plaques on the Extensor Surfaces
Introduction. A 59-year-old woman with Fitzpatrick skin type V presented to the dermatology clinic with symmetrically distributed brown plaques on the extensor surfaces of her knees, elbows, proximal interphalangeal (PIP) joints, and metacarpophalangeal (MCP) joints.
History. The patient first noticed the asymptomatic lesions 1 month prior to presentation. The patches were dark brown, thin (Figure 1) and symmetrically distributed over her elbows, knees, PIP joints, and MCP joints (Figure 2).

Figure 1. The patient presented with patches that were dark brown, thin, and symmetrically distributed.

Figure 2. The patches were distributed over her elbows, knees, proximal interphalangeal joints, and metacarpophalangeal joints.
She denied associated pruritus or pain but endorsed mild, chronic stiffness in the wrists and PIP joints. The patient reported a family history of systemic lupus erythematosus (SLE) in multiple second-degree relatives.
She worked in an office setting and spent most of her day typing at a desk, frequently resting her elbows on the hard surface. Prior to presentation, she began using triamcinolone 0.025% cream on the plaques, as advised by her primary care provider, with partial improvement in pigmentation.
Physical examination revealed dark brown, thin plaques on the extensor surfaces of the bilateral knees, elbows, MCP, PIP, and metatarsophalangeal (MTP) joints. There was no erythema or scale.
Diagnostic Testing. A 3 mm punch biopsy of a representative hyperpigmented plaque on the left elbow (Figure 3) was stained with hematoxylin and eosin (H & E).

Figure 3. A biopsy was taken of the hyperpigmented plaque on the patient’s right elbow.
Histopathology, shown at 10x (Figure 4), 40x (Figure 5), and 100x magnification (Figure 6), demonstrated epidermal papillomatosis, hyperkeratosis, and hypergranulosis without interface dermatitis or significant inflammation. After testing, the patient was diagnosed with Frictional Asymptomatic Darkening of the Extensor Surfaces (FADES).
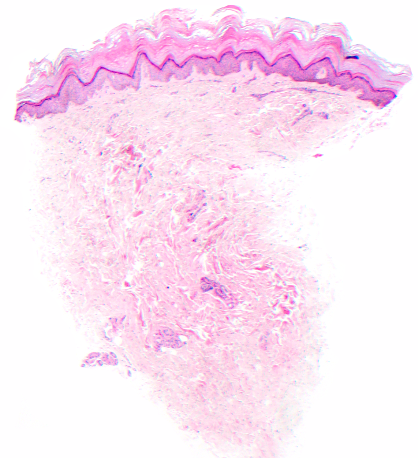
Figure 4. Histopathology, H & E stain, shown at 10x.
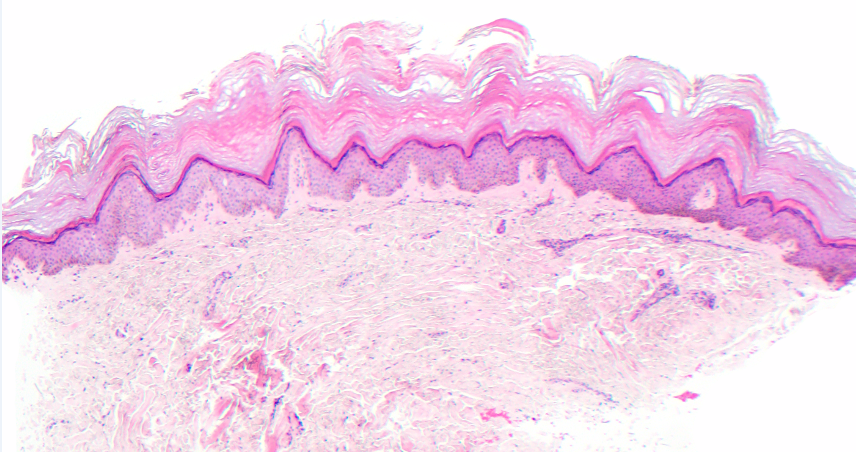
Figure 5. Histopathology, H & E stain, shown at 40x.
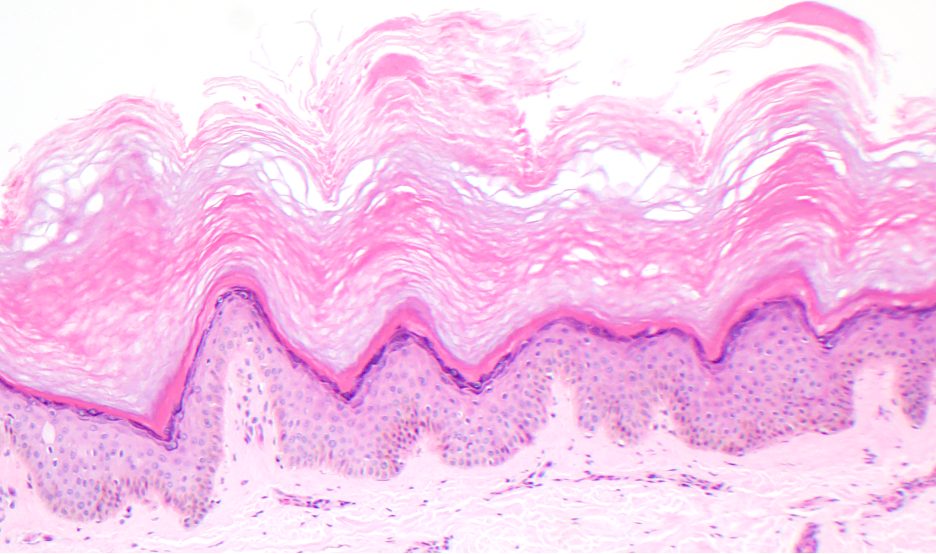
Figure 6. Histopathology, H & E stain, shown at 100x.
Differential diagnoses. Several conditions were considered in the differential diagnosis of this patient’s hyperpigmented plaques. Post-inflammatory hyperpigmentation (PIH) was initially considered due to the brown discoloration and the patient’s Fitzpatrick skin type V. We considered PIH because it is classically more prevalent and pronounced in individuals with darker skin tones. However, the patient did not report any preceding inflammation, significant trauma, or dermatologic condition, and histopathology did not demonstrate melanin deposition in the dermis, a hallmark finding in PIH.1
Contact dermatitis was also considered because of the plaque distribution over areas that the patient reported contacting environmental surfaces, such as a desk or clothing. However, the patient denied exposure to new products or allergens, and there were no symptoms of pruritus, erythema, or vesiculation. Histopathologic evaluation further ruled this out by showing no spongiosis or inflammatory infiltrate, which are typically seen in allergic or irritant contact dermatitis.1
Lichen simplex chronicus (LSC) was a plausible differential, given the presence of hyperpigmented plaques and a potential history of mechanical friction. However, the patient reported no pruritus or habitual scratching of the affected areas. LSC is typically associated with thickened skin due to chronic scratching, and histology often shows acanthosis, hypergranulosis, and a lymphocytic infiltrate.1 These symptoms were absent in this case.
Psoriasis vulgaris was considered because of the symmetric distribution on extensor surfaces, a classic feature of the condition. However, this diagnosis was unlikely due to the absence of characteristic silvery scale, erythema, or a personal or family history of psoriasis, along with histologic findings that lacked parakeratosis, neutrophilic microabscesses, or elongated rete ridges.1
Given the patient's fatigue, joint stiffness, and family history of SLE, connective tissue diseases—particularly dermatomyositis—were also considered. In patients with darker skin types, dermatomyositis may present as hyperpigmented patches rather than the typical violaceous hue seen in lighter skin.4 However, the absence of systemic symptoms such as muscle weakness, heliotrope rash, Gottron’s papules, or poikiloderma, along with a skin biopsy that showed no interface dermatitis or mucin deposition, argued against this diagnosis.1 The biopsy was also helpful in ruling out SLE and other connective tissue disorders that typically show interface dermatitis and mucin deposition.
Treatment and management. The patient was counseled on avoiding frictional triggers such as prolonged resting of elbows or knees on hard surfaces. She was prescribed tazarotene 0.1% cream to be applied daily to the affected areas. Topical keratolytic agents such as urea or lactic acid were discussed as adjuncts, although not initiated at this time.
Outcome and follow-up. The patient’s initial response to triamcinolone cream prior to dermatology consultation led to some reduction in pigmentation. 3 months later at follow-up, she reported adherence to topical therapy and environmental modifications. No adverse effects were noted. She was advised that FADES is a benign but chronic condition and that cosmetic improvement may be gradual. Long-term management would focus on friction avoidance and consistent topical treatment.
Discussion. FADES is an uncommon dermatologic condition characterized by uniform, asymptomatic brown patches or thin plaques, most commonly found on the extensor surfaces of the elbows and knees.1,2 Patients typically present with hyperpigmented lesions with minimal scaling without pruritus, pain, or inflammation.1 A history of repeated frictional stress to the affected areas should raise clinical suspicion for FADES.1 For example, dark patches on the knees in someone who frequently kneels while gardening, or, as demonstrated in this case, darkening of the elbows in an office worker who rests her elbows on a desk while typing.
Although similar cases had been described previously, FADES was first formally defined as a distinct clinical entity by Krishnamurthy et al. in 2005.1,2 Unlike PIH, FADES does not involve melanin deposition in the dermis.1 Instead, the darkened brown patches are a result of epidermal hyperkeratosis secondary to chronic frictional stress.1 Patient history is often useful in ruling out alternative diagnoses like contact dermatitis, lichen simplex chronicus, psoriasis vulgaris and connective tissue disorders.
Dermoscopy findings in FADES have not been extensively characterized, but reported features include sparse, brownish, uniformly sized clods partially interconnected by fine white lines.2 While clinical features and patient history are often enough to reach the diagnosis of FADES, biopsy remains the definitive standard for confirming FADES, particularly when the presentation overlaps with other dermatologic conditions. Histologically, the hyperpigmented-appearing plaques of FADES are hyperkeratotic without increased melanin.1 A biopsy consistent with FADES demonstrates papillomatosis with acanthosis, marked hyperkeratosis, and an absence of inflammation.1 The lack of inflammation in FADES is helpful to differentiate from other entities in the clinical differential diagnosis.1
Several case reports have provided insight into the presentation of FADES in patients with lighter skin tones, but documentation of FADES in patients with Fitzpatrick skin type V or darker remains limited. Early descriptions referred to the condition as the “sign of dirty knees and elbows,” reflecting patients’ complaints of the visual resemblance of the lesions to dirt.3 However, in patients with darker skin, this sign or complaint may be less apparent due to reduced contrast between the affected and surrounding skin. In our patient with Fitzpatrick type V skin, the diagnosis of FADES was best supported by the presence of asymptomatic, uniform dark patches, a clear history of frictional stress, and biopsy findings of hyperkeratosis and papillomatosis with acanthosis. Biopsy was particularly helpful in this case to exclude dermatomyositis and psoriasis in the setting of joint pain.
Management of FADES typically includes the use of topical keratolytic agents such as lactic acid or urea cream, which help reduce the hyperkeratotic thickening of the lesions.1 Avoidance of frictional triggers is also key to preventing progression.1 These treatments are generally safe for all skin types, provided the topical medications are applied only to the affected areas and monitored for potential irritation or PIH.4 Our patient’s treatment plan includes avoidance of frictional stressors and tazarotene 0.1% cream applied to affected areas daily. While FADES is a benign condition, it is chronic, and therefore, patient counseling should focus on setting realistic expectations regarding cosmetic improvement and continual management. 1
Conclusion. FADES should be considered in patients presenting with symmetric, asymptomatic, hyperpigmented plaques on extensor surfaces, especially when in conjunction with a history of frictional stress. Biopsy is most helpful in distinguishing this condition from other pigmented dermatoses, particularly in patients with darker skin types.
AUTHORS:
Ella Tiller, BS1 • Russell Newkirk, MD2 • Ari Gelman, MD2
AFFILIATIONS:
1Uniformed Services University of the Health Sciences, Bethesda, MD
2Walter Reed National Military Medical Center, Bethesda, MD
CITATION:
Tiller E, Newkirk R, Gelman A. Hyperpigmented plaques on the extensor surfaces. Consultant. Published online November 19, 2025. doi:10.25270/con.2026.01.000005
Received July 8, 2025. Accepted Sep. 4, 2025.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE:
Russell Newkirk, MD, Walter Reed National Military Medical Center, 4301 Jones Bridge Rd, Bethesda, MD 20814 (egtiller@gmail.com)
References
- Krishnamurthy S, Sigdel S, Brodell RT. Frictional asymptomatic darkening of the extensor surfaces. Cutis. 2005;75:349-355.
- Tan C, Xia L. Dermoscopy of frictional asymptomatic darkening of the extensor surfaces. Postepy Dermatol Alergol. 2019 Apr;36(2):232-233. doi:10.5114/ada.2019.84598.
- Ber A. The sign of dirty knees and elbows. Acta Endocrinol (Copenh). 1954;16:305–8. doi:10.1530/acta.0.0160305.
- Abdel Meguid AM, Elaziz Ahmed Attallah DA, Omar H. Trichloroacetic acid versus salicylic acid in the treatment of acne vulgaris in dark-skinned patients. Dermatol Surg. 2015 Dec;41(12):1398-404. doi:10.1097/DSS.0000000000000522.
©2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Consultant360 or HMP Global, their employees, and affiliates.