
Peer Reviewed
Daptomycin-Induced Eosinophilic Pneumonia in a Rural Setting
Introduction. A 46-year-old man presented to the emergency department with shortness of breath, fluctuating blood pressure, tachycardia, and a mild fever (< 100℉).
History. The patient had a history of schizophrenia, anxiety, type 2 diabetes mellitus, stage 3 chronic kidney disease, hypertension, hyperlipidemia, and Charcot foot. His past hospitalizations included a recent admission at another facility for bone debridement and external fixation of the left lower extremity due to methicillin-resistant staphylococcus aureus (MRSA)-associated osteomyelitis of his Charcot foot. It was during this time that the patient was also found to have MRSA bacteremia. During that hospitalization, the patient was prescribed 1500mg IV vancomycin BID for a total of 6 weeks to resolve his MRSA infection. After 6 days, he was discharged; set to complete the remaining infusions at home via a home health care company. He was then hospitalized again 6 days later at a second facility due to a presumed acute kidney injury (AKI) caused by vancomycin. During that hospitalization, a period of 3 days, the patient was treated for his AKI and transitioned from vancomycin to 700mg IV daptomycin daily for a total of 30 days. His arrival at our hospital with the above presentation came 6 days after the resolution of his AKI and discharge from that hospital.
On physical examination, O₂ saturation was 87% on room air, heart rate was 115 beats/min, respiratory rate was 19 breaths/min, blood pressure was 118/97 mm Hg, and temperature was 99.9℉. Diffuse bilateral crackles were noted in all lung fields. The patient met criteria for sepsis and was briefly transferred to the intensive care unit due to hypotension (blood pressure of 72/54 mm Hg) and worsening respiratory distress.
Diagnostic Testing. The patient’s chest x-ray (CXR; Figure 1) and computed tomography angiography (CTA; Figure 2) confirmed the presence of diffuse infiltrates across both lungs, and mediastinal and perihilar adenopathy.
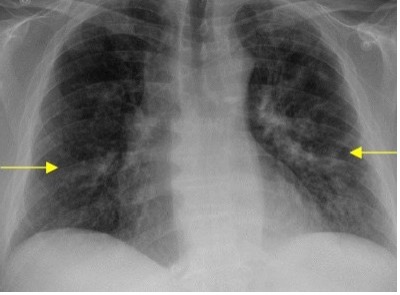
Fig. 1. Portable CXR illustrating areas of diffuse pulmonary infiltration (yellow arrows).

Fig. 2. Transverse view of chest CTA illustrating multiple areas of ground glass consolidation (black arrows).
Previous CXR from the patients’ past hospitalizations indicated no previous pulmonary infiltration. Further laboratory studies revealed a white blood cell count of 13,700/µL (normal range: 4500 - 11,000/ µL) with an eosinophilic predominance of 9.8% (normal range: 1-4%).
While being treated for septic shock, clinical suspicion of daptomycin-induced eosinophilic pneumonia (DIEP) was raised. Once stabilized through the hospital’s sepsis protocol, the patient’s current onset of symptoms was confirmed to have occurred after the transition to daptomycin. Given these findings, DIEP became the working diagnosis within the first 24 hours of the patients’ hospitalization.
Differential Diagnosis. A diagnosis of MRSA pneumonia could have easily been just as credible given his recent diagnosis of MRSA bacteremia. Given this complex and overlapping differential, early discovery of his recent medication change, noted eosinophilic leukocytosis, and a positive intervention with a steroid therapy were key to finalizing a diagnosis of DIEP.
Treatment and Management. The patient was transitioned from daptomycin to linezolid 600 mg twice a day and began intravenous methylprednisolone 40 mg three times daily. Within the next 24 hours, the patient demonstrated rapid improvement. Specifically, repeat CXRs showed improved pulmonary infiltration, the patient was able to be gradually weaned to room air with O₂ saturation in the 90s, and the patient’s eosinophilia had declined significantly with a white blood cell count of 10,800/µL (Normal range, 4500 - 11,000/ µL) and a 0.7% (normal range: 1-4%) eosinophil predominance. This medication regimen was continued for 4 days before the IV solumedrol was transitioned to prednisone in anticipation of his discharge, which occurred 1 week after his admission.
Outcome and Follow-up. At the time of discharge, the patient had been stable on room air with O₂ saturations of 93% to 96%, his white blood cell count was no longer significant for leukocytosis at 7,400/µL with a 1.1% eosinophil predominance, and he reported a resolution of his respiratory symptoms. The patient was started on an oral prednisone taper consisting of 40mg for 5 days, 30mg for the next 5 days, and 20mg over the remaining 5 days, and was given a follow up appointment to Pulmonology at discharge. The patient’s lung fields were notably improved on auscultation and repeat CXRs showed improvement of the infiltration noted on admission (Figure 3).
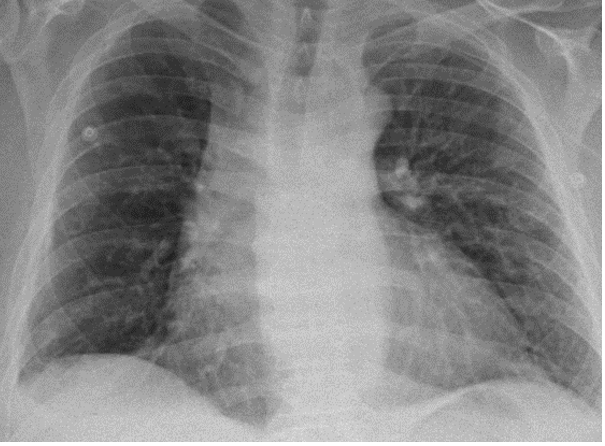
Fig. 3. Portable CXR illustrating stable/improved pulmonary infiltration after the initiation of steroid therapy.
Discussion. Daptomycin has seemingly cemented its place as a front-line empiric antibiotic in the setting of severe infection with a gram-positive organism and as a second-line therapy in situations where the initial agent is no longer feasible due to resistance or allergy.3,4,6 Specifically, its gram-positive activity makes it useful in the treatment of MRSA and vancomycin-resistant enterococcus spp (VRE) infection.2,5,7 Unfortunately, this degree of coverage is somewhat eclipsed by reports of severe pulmonary toxicity that can lead to acute respiratory distress syndrome.1,8 Daptomycin is, in fact, the leading cause of drug-induced eosinophilic pneumonia.1 This report highlights a case of DIEP diagnosed and managed within a rural hospital setting without the use of specialist care. As detailed above, the discontinuation of daptomycin in the treatment of MRSA bacteremia in favor of linezolid and steroid therapy resulted in the resolution of the patient’s respiratory symptoms.
Fortunately, this reaction is generally rare; with some sources estimating an incidence of less than 5%,1 which could explain why this adverse reaction is poorly understood. Another reasoning might be that the illness is promptly reversed with a transition away from the offending agent and the application of a steroid therapy.1,8 Regardless, the need for good clinical insight is apparent given the generalized nature of the presenting symptoms including cough, respiratory distress, novel and diffuse infiltrates seen with imaging, possible fever, and the novel initiation of daptomycin.1,8 Several characteristics have, however, been noted as predisposing factors that may aid in the clinical identification of this illness, including the male sex, hypertension, baseline renal dysfunction, individuals older than 70 years of age, or individuals who have maintained a daptomycin regimen equal to or longer than 14 days. Currently, it is unclear whether a daptomycin regimen which -in total- amounts to 10 or more grams predisposes a patient to this reaction. Regardless, patients typically present with symptoms two to four weeks after the initiation of daptomycin -with a smaller subset presenting subacutely at 5 months. In addition to the symptoms noted above, patients may also present with bilateral crackles on chest auscultation, or signs suggestive of pleural effusions.1
Interestingly, this patient arrived with a cough, respiratory distress, diffuse infiltrates on CXR and CTA, as well as a fever and bilateral crackles heard with auscultation only 6 to 7 days after his initiation of daptomycin. This is a slight departure from the expected time to presentation of 2 to 4 weeks noted previously. Fortunately, his recent initiation of a daptomycin regimen, clinical presentation, and white count differential showcasing eosinophilic leukocytosis lent a great degree of credulity to a diagnosis of DIEP.
An additional clinical step that we could have taken would have been a bronchioalveolar lavage (BAL); diagnostically confirming daptomycin-induced eosinophilic pneumonia should the lavage reveal >25% eosinophils within the lung.1 However, due to the rural nature of our hospital, pulmonology service was unavailable at the time of presentation, and our suspicions were confirmed via patient improvement after treatment for DIEP. The perceived improvement included a stable shift from oxygenation to room air, improved chest infiltration as seen with repeat CXRs, decreased eosinophilia, and a remission of his presenting symptoms.
This resolution despite adverse circumstances—specifically those where support from specialized physicians is unavailable—underlines the need for prompt recognition and treatment of less common disease processes in a rural setting. Traditionally, a case of DIEP might be handled in the setting of an educational hospital or one of a higher acuity where these services are regularly available. However, as noted previously, a delay in the diagnosis and treatment of DIEP could lead to an instance of acute respiratory distress. A progression made more serious in the case of this patient who was already presenting with signs and symptoms of septic shock. In this instance the patient’s presentation and a thorough understanding of DIEP allowed for the resolution of this acute event in a rural setting without the use of the gold standard BAL or the utilization of a pulmonologist.
DIEP is a noted rarity within the field of medicine. However, despite its absence from the day-to-day clinical workup, its clinical features must be within the mind of physicians as its progression toward acute respiratory distress makes it a must-not-miss diagnosis. Patients presenting with respiratory symptoms after being initiated on a daptomycin therapy should immediately fall under this consideration. Fortunately, timely recognition of DIEP and the discontinuation of daptomycin in favor of an alternative antibiotic and steroid therapy has proved sufficient to reverse much of the disease’s progression. While this change is typically achieved in the setting of urban medicine, this report illustrates that this condition can be appropriately managed in even a rural setting given physician awareness.
AUTHOR:
Thomas Eggleston, BS1
AFFILIATIONS:
1Osteopathic Medical Student (OMS) III, The Kentucky College of Osteopathic Medicine, Pikeville, KY
CITATION:
Eggleston T. Daptomycin-induced eosinophilic pneumonia in a rural setting. Consultant. Published online May 15, 2025. doi: 10.25270/con.2025.05.000001
Received October 31, 2024. Accepted January 2, 2025.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
Thanks to Bryant Dawson, DO, who was my mentor throughout the case.
CORRESPONDENCE:
Thomas Eggleston, BS, 147 Sycamore St, Pikeville, KY 41501, (Thomaseggleston@upike.edu)
References:
- Abbott IJ, Cairns KA. Daptomycin: an overview. UpToDate. Published September 2024. Accessed October 28, 2024. https://www.uptodate.com/contents/daptomycin-an-overview
- File TM Jr. Treatment of community-acquired pneumonia in adults. UpToDate. Published September 2024. Accessed October 28, 2024. https://www.uptodate.com/contents/treatment-of-community-acquired-pneumonia-in-adults
- Fowler VG, Boucher HW, Corey GR, et al. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. N Engl J Med. 2006;355(7):653-665. doi:10.1056/NEJMoa053783. Accessed October 28, 2024.
- Holland TL, Arnold C, Fowler VG. Clinical management of Staphylococcus aureus bacteremia. JAMA. 2014;312(13):1330-1341. doi:10.1001/jama.2014.9743. Accessed October 27, 2024.
- Klompas M. Treatment of hospital-acquired and ventilator-associated pneumonia in adults. UpToDate. Published September 2024. Accessed October 29, 2024. https://www.uptodate.com/contents/treatment-of-hospital-acquired-and-ventilator-associated-pneumonia-in-adults
- Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18-e55. doi:10.1093/cid/ciq146. Accessed October 29, 2024.
- Lowy FD. Methicillin-resistant Staphylococcus aureus (MRSA) in adults: treatment of bacteremia. UpToDate. Published September 2024. Accessed October 28, 2024. https://www.uptodate.com/contents/methicillin-resistant-staphylococcus-aureus-mrsa-in-adults-treatment-of-bacteremia
- Portalatin GM, Chin JA, Foster B, Perry K, McWilliams C. Daptomycin-induced acute eosinophilic pneumonia. Cureus. 2021;13(2):e13509. doi:10.7759/cureus.13509. Accessed October 28, 2024.