
Peer Reviewed
Bilateral Bladder-Containing Inguinal Hernias Incidentally Detected on Voiding Cystorethogram in a Pre-Term Infant
Introduction. A 2-month-old infant in the neonatal intensive care unit (NICU), born at 24 weeks and 1 day of gestation, presented for evaluation of recurrent urinary tract infections (UTI).
History. The patient’s course in the NICU was complicated by prematurity-related conditions such as bronchopulmonary dysplasia and neonatal pneumonia. At 6 weeks prior to his presentation, he developed a Klebsiella UTI that improved with antibiotic therapy. At 1 week before the current evaluation, he again experienced a Klebsiella UTI accompanied by clinical signs of sepsis and underwent another 7-day treatment course with IV cefepime 50mg/kg twice a day. His persistent and recurrent UTIs prompted further imaging investigation to identify an underlying anatomical cause.
Diagnostic Testing. Catheterized urine cultures confirmed more than 100,000 colony-forming units of Klebsiella on two separate occasions. A renal and bladder ultrasound (RBUS) initially showed mild left-sided hydronephrosis, a minimally distended bladder, and otherwise normal renal parenchyma. He then underwent a voiding cystourethrogram (VCUG) for further assessment of the urinary tract, which incidentally revealed bilateral bladder herniations into the inguinal canals, without vesicoureteral reflux or urethral anomalies (Figure 1). The bladder emptied nearly completely at the end of the study with spontaneous bladder-containing inguinal hernias resolution.
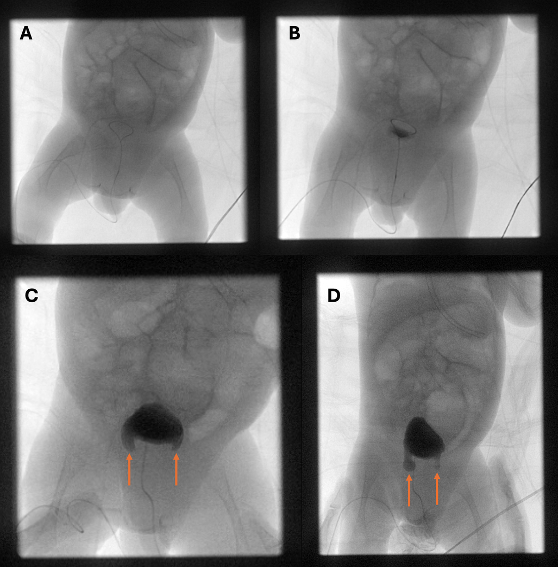
Figure 1. Voiding cystourethrogram: (A) scout image without contrast; (B) partial bladder filling with no apparent abnormality; (C, D) bilateral bladder containing inguinal hernias, no vesicoureteral reflux.
Differential diagnosis. Recurrent UTIs in a male infant raise suspicion for congenital genitourinary anomalies. Vesicoureteral reflux (VUR), posterior urethral valves (PUV), ureteropelvic junction (UPJ) obstruction, and neurogenic bladder can all lead to urinary stasis and infection. Each of these conditions typically exhibits distinct imaging or clinical findings: VUR is characterized by retrograde flow of urine to the renal collecting system on VCUG, PUV involves an obstructive membranous fold in the posterior urethra with resultant bilateral hydronephrosis, UPJ obstruction impedes urine flow from the kidney to the bladder, and neurogenic bladder arises from spinal cord or nerve abnormalities that impair normal bladder emptying. Imaging findings were not consistent with any of these possibilities. Instead, the bilateral inguinal herniation of the bladder floor was incidentally identified, which can be a cause of urinary stasis and predispose to recurrent infection.
Treatment and management. After completing 7-day course of cefepime, the patient was treated for other conditions of prematurity in the in the NICU. After approximately 6 weeks of management and optimization, the pediatric urology team proceeded with bilateral indirect inguinal hernia repairs. Intraoperatively, both hernia sacs containing portions of the bladder were identified, reduced, and repaired. A circumcision was performed concurrently. Postoperative pain was controlled with intravenous acetaminophen 15mg/kg q6h PRN (5 total doses administered), and the infant remained hemodynamically stable throughout his recovery as the patient remained afebrile and without tachycardia. NICU-level care was continued as the patient continued to require active management of his chronic lung disease, retinopathy of prematurity, anemia of prematurity, and low birth weight. For treatment of the respective conditions, he required alternating doses of Atrovent and Pulmicort q12h (one administered every 6 hours); dorzolamide, timolol, latanoprost; a daily multivitamin with iron; and Neosure 27cal/oz. Each of these active conditions were stabilized following his surgery and he was discharged from the NICU on post-operative day 5.
Outcome and follow-up. Throughout the 5-day post-operative period, the patient was not noted to experience any UTI sequelae or new infectious episodes. stay. At the time of discharge, the patient’s duration-of-stay was nearly 4 months. Discharge planning included planned pediatric urology follow-up 4-6 weeks following discharge, with repeated ultrasound imaging recommended prior to the next outpatient visit for evaluation of the surgical repair site and renal status. At his 4-week patient follow-up, the patient was found to be doing well. Retroperitoneal ultrasound was obtained at that visit which showed normal appearance of the kidneys with a decompressed urinary bladder. The patient was instructed to follow up again in 1-2 months after this appointment. Upon that visit 2 months later, retroperitoneal ultrasound was again obtained and showed normal appearing bladder and kidneys bilaterally. He has not required readmission for UTI or other genitourinary issues since the hernia repair. The surgical correction of these rare bladder-containing hernias appears to have mitigated his recurrent UTIs and improved his overall clinical trajectory.
Discussion. Inguinal hernias in infants generally arise from a patent processus vaginalis, which fails to close and allows abdominal or pelvic contents to protrude into the inguinal canal. Elevated intra-abdominal pressure can exacerbate this predisposition, particularly in preterm infants who often have underdeveloped connective tissues within the abdominal wall, which provide less structural support.1,10 While 3% to 5% of full-term infants experience an inguinal hernia, the incidence among preterm infants is significantly higher, and ranges up to 30% depending on birth weight and gestational age. Bladder involvement within an inguinal hernia is particularly rare and occurs in approximately 1% to 4% of inguinal hernia cases.1-6 The role of a bladder-involved inguinal hernia in the development of UTIs is not definitively established; however, herniation of a portion of the bladder may alter urinary dynamics, potentially leading to stasis and subsequently presenting with signs of urinary dysfunction such as recurrent UTIs or urinary retention.11 These are generally surgically repaired considering the risk for incarceration and strangulation.7,8 Voiding cystourethrogram, an imaging study that outlines the bladder and urethra during filling and emptying, can incidentally reveal these hernias when investigating recurrent UTIs or other urinary anomalies.
In our patient, recurrent Klebsiella UTIs prompted further evaluation and revealed bilateral bladder-containing inguinal hernias in the absence of other anatomic abnormalities. Given the risks of incarceration and possible urinary dysfunction, surgical repair was deemed necessary, and in this case, was followed by resolution of UTIs.
AUTHORS:
Carl David Pfaehler, BA1 • Kevin Pierre, MD2 • Cing Hoih3 • Mariana Rodero Cardoso, MD4
AFFILIATIONS:
1University of Florida College of Medicine
2University of Florida Department of Radiology
3University of Florida College of Liberal Arts and Sciences
4University of Florida Department of Radiology, Division of Pediatric Radiology
CITATION:
Pfaehler CD, Pierre K, Hoih C, Rodero Cardoso M. Bilateral bladder-containing inguinal hernias incidentally detected on voiding cystourethrogram in a preterm infant. Consultant. Published online: July 14, 2025. DOI:10.25270/con.2025.07.000001
Received March 2, 2025. Accepted April 8, 2025.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE:
Mariana Rodero Cardoso, MD, 1600 SW Archer Rd., Gainesville, FL 32608 (mrib0001@radiology.ufl.edu)
References
- Burgmeier C, Dreyhaupt J, Schier F. Comparison of inguinal hernia and asymptomatic patent processus vaginalis in term and preterm infants. J Pediatr Surg. 2014;49(9):1416-1418. https://doi.org/10.1016/j.jpedsurg.2014.04.018
- Fu YW, Wang LY, Tiao MM, et al. A nationwide survey of incidence rates and risk factors of inguinal hernia in preterm children. Pediatr Surg Int. 2018;34(1):91-95. https://doi.org/10.1007/s00383-017-4186-6
- Kumar VH, Clive JM, Rosenkrantz TS, et al. Inguinal hernia in preterm infants (≤32-week gestation). Pediatr Surg Int. 2002;18(2-3):147-152. https://doi.org/10.1007/s003830100651
- DeCou JM, Gauderer MW. Inguinal hernia in infants with very low birth weight. Semin Pediatr Surg. 2000;9(2):84-87. https://doi.org/10.1053/spsu.2000.6751
- Harper RC, Garper A, Sia CN. Inguinal hernia: a common problem of premature infants weighing 1,000 grams or less at birth. Pediatrics. 1975;56(1):112-115.
- Bisharat M, O’Donnell ME, Thompson T, et al. Complications of inguinoscrotal bladder hernias: a case series. Hernia. 2009;13(1):81-84. https://doi.org/10.1007/s10029-008-0434-0
- Kapisiz A, Ozcan S, Ozturk H, et al. Our cases and literature review for presence of bladder hernias in the inguinal region in children. Diagnostics (Basel). 2023;13(9):1521. https://doi.org/10.3390/diagnostics13091521
- Manatt S, Templeton T, Frimberger D, et al. Inguinal herniation of the bladder in an infant. Can J Urol. 2006;13(2):3057-3058.
- Hoberman A, Wald ER, Hickey RW, et al. Imaging studies after a first febrile urinary tract infection in young children. N Engl J Med. 2003;348(3):195-202. https://doi.org/10.1056/NEJMoa021698
- Sharma S, Curry J. Inguinal hernia in premature infants. J Indian Assoc Pediatr Surg. 2015;20(1):25-26. https://doi.org/10.4103/0971-9261.145438
- Kraft KH, Sweeney DD, Clemens JQ, et al. Inguinoscrotal bladder hernias: report of a series and review of the literature. Can Urol Assoc J. 2008;2(6):619-623. https://doi.org/10.5489/cuaj.982