
Peer Reviewed
Air Embolism to the Anterior Spinal Artery Secondary to Percutaneous Lung Biopsy
Introduction. A 63-year-old man developed acute bilateral lower extremity weakness and numbness immediately following a percutaneous lung biopsy.
History. The patient had a medical history significant for invasive squamous cell carcinoma of the skin and presented with a new right lower lobe (RLL) lung mass. A prior bronchoscopy for the lung mass was inconclusive and led to a referral for a computed tomography (CT)-guided percutaneous transthoracic biopsy by interventional radiology (Figure 1).
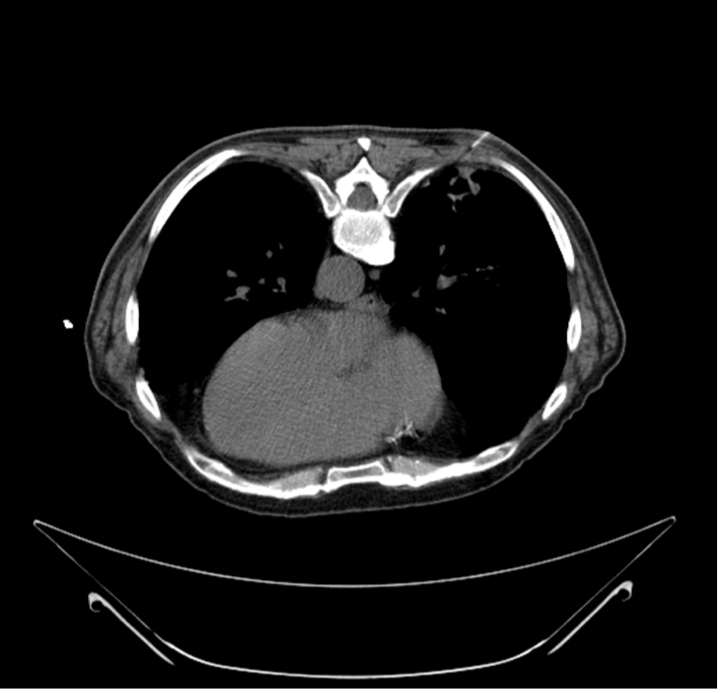
Figure 1. The biopsy needle penetrating the right lower lobe lung mass during CT-guided lung biopsy. The patient was in the prone position.
Immediately after the biopsy procedure, the patient experienced sudden onset of bilateral lower extremity weakness and numbness. He was unable to move his legs and exhibited signs consistent with acute paraplegia.
Physical examination. On examination, the patient was alert and oriented, with a respiratory rate of 20 breaths per minute and oxygen saturation of 97% on room air. Decreased breath sounds were noted at the right lung base. Neurological examination revealed paraplegia with complete motor loss in both lower extremities. Sensory examination showed decreased sensation in the lower extremities bilaterally. There were no changes in speech or cognition.
Diagnostic testing. A CT scan performed immediately after the biopsy identified a small pneumothorax that did not require chest tube placement at the biopsy site (Figure 2).
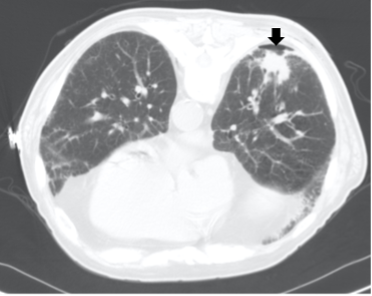
Figure 2. CT scan showing a small loculated pneumothorax (black arrow) at the biopsy site post-procedure.
Additionally, CT imaging demonstrated air within the anterior spinal canal (Figure 3A), the descending thoracic aorta (Figure 3B), and the left ventricle of the heart (Figure 3C). Minute amounts of air were also noted in the left subcostal vessels. A CT scan of the brain showed no evidence of air emboli in the cerebral vasculature or intracranial hemorrhage.
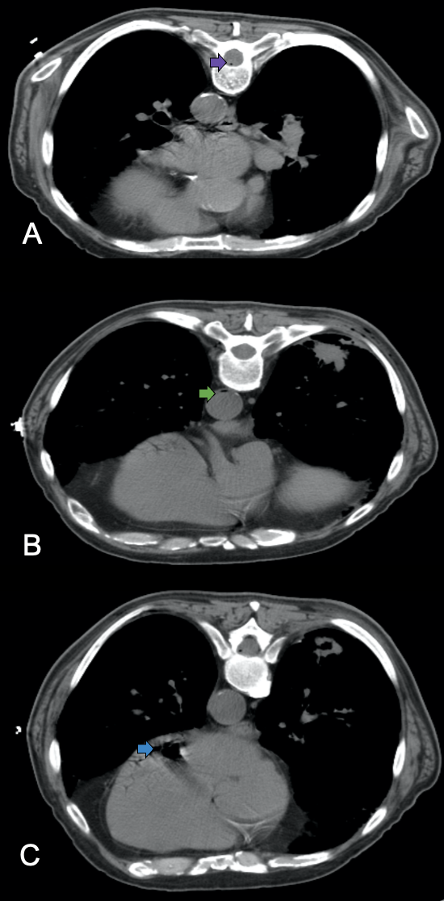
Figure 3. (A) Axial CT demonstrates a small air bubble in the anterior spinal canal (purple arrow), indicative of air in the anterior spinal artery. (B) Axial CT shows air bubbles in the descending thoracic aorta (green arrow). (C) CT reveals an anti-dependent air pocket within the left ventricle of the heart (blue arrow).
Differential diagnoses. The sudden onset of paraplegia following the percutaneous lung biopsy prompted consideration of several differential diagnoses. Potential causes included arterial air embolism causing spinal cord ischemia, spinal cord infarction due to thromboembolism, epidural hematoma, direct trauma to the spinal cord, and acute transverse myelitis. Given the imaging findings of air in the anterior spinal canal and systemic arterial circulation, we diagnosed the patient with an arterial air embolism to the anterior spinal artery as the cause of the spinal cord ischemia.
Treatment and management. Immediate management focused on stabilizing the patient and preventing further neurological damage. The patient was placed in the Trendelenburg position to reduce cerebral air embolism risk and administered 100% oxygen to promote the absorption of intravascular air bubbles. We also promptly initiated hyperbaric oxygen therapy to reduce the size of air emboli and improve oxygen delivery to ischemic tissues. The patient was airlifted to a facility equipped for hyperbaric oxygen therapy, which he received for 4 days.
Outcome and follow-up. During the next 30 minutes following initial management, and before transfer for hyperbaric oxygen therapy, the patient noted improvement in his symptoms and regained strength in his lower extremities. Despite experiencing urinary retention requiring an indwelling Foley catheter, his motor function continued to improve.
At an outpatient follow-up visit that occurred after hospital discharge, the patient reported significant recovery of motor skills, balance, strength, and ambulation, though he continued to use a cane for assistance and performed intermittent self-catheterization due to residual bladder dysfunction. The lung biopsy results confirmed malignancy. A follow-up CT scan of the brain, performed and reviewed during the outpatient follow-up visit, showed no concerning findings.
Discussion. Arterial air embolism is a rare but potentially fatal complication of percutaneous lung biopsy, with a clinically apparent incidence ranging from 0.02% to 0.07%, although undetected cases may increase this rate up to 3.8%.1-2 Prompt recognition and intervention can mitigate morbidity and mortality associated with this condition.3-5 However, arterial air embolism may occasionally be missed on initial CT imaging, particularly if small intravascular air bubbles are overlooked or imaging is not performed immediately post-procedure. Careful inspection of the aorta, coronary arteries, cerebral circulation, and spinal vasculature on early post-biopsy imaging can improve detection.2,3
The mechanism of arterial air embolism involves the introduction of air into the pulmonary venous circulation when the biopsy needle traverses both the bronchi and pulmonary veins. The negative intrathoracic pressure generated during inspiration creates a pressure gradient between which facilitates air entry into the vasculature.4,6 Air emboli can then travel from the pulmonary veins to the left heart and systemic arterial circulation, where they can lodge in critical vasculature such as the cerebral or spinal arteries.6
Clinical manifestations depend on the volume of air embolized, the target vessel, and the organ supplied. Neurological deficits, including spinal cord ischemia and paraplegia, can occur when air emboli occlude spinal arteries.7-9 In this case, the patient's immediate onset of paraplegia was indicative of anterior spinal artery ischemia.
Management includes immediate supportive measures: securing the airway, providing high-flow oxygen, and improving hemodynamics.3,5,9 Patient positioning, such as the Trendelenburg position, may help prevent cerebral embolization.9 Hyperbaric oxygen therapy is recommended within 4 to 6 hours of symptom onset, as it reduces bubble size and increases oxygen delivery to ischemic tissues. Delay beyond the 4 to 6 hours of window may reduce its efficacy, as prolonged hypoxia can lead to irreversible tissue injury.4,10
Prevention strategies during percutaneous lung biopsy involve specific techniques to minimize the risk of air embolism. Specific techniques include the use of coaxial biopsy systems with hemostatic valves, which help prevent air ingress during instrument exchange. 8,10 Clinicians should also avoid traversing bullae, cavitary lesions, or cystic lung regions, as these structures may contain pressurized air and increase the risk of air entering the pulmonary veins.10,11 Performing the biopsy during a breath-hold at end-expiration helps reduce intrathoracic pressure, thereby limiting the pressure gradient that drives air into the vasculature.10 Additionally, minimizing the number of pleural punctures and reducing needle dwell time further lowers the risk of systemic air embolism.11
Conclusion. Arterial air embolism to the anterior spinal artery is a rare but serious complication of percutaneous lung biopsy. Clinicians should be aware of this potential adverse event and maintain a high index of suspicion in patients presenting with acute neurological deficits post-procedure. Immediate management with supportive measures and hyperbaric oxygen therapy can result in favorable outcomes, as demonstrated in this case.
AUTHORS:
Amanda Acevedo, BS¹ • Rajvi Thakkar, BS¹ • U. George McCann III, MD¹ • Kevin Pierre, MD² • Damodaran Arulselvam, MD³
AFFILIATIONS:
¹College of Medicine, University of Florida, Gainesville, FL
²Department of Radiology, University of Florida, Gainesville, FL
³North Florida/South Georgia Veterans Health System, Gainesville, FL
CITATION:
Acevedo A, Thakkar R, McCann GU III, et al. Consultant. Published online July 21, 2025. doi: 10.25270/con.2025.07.000006
Received October 27, 2024. Accepted March 8, 2025
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Amanda Acevedo, BS, 1600 SW Archer Road, Gainesville, FL 32601 (Email: amanda.acevedo@ufl.edu)
References
- Freund MC, Petersen J, Goder KC, Bunse T, Wiedermann F, Glodny B. Systemic air embolism during percutaneous core needle biopsy of the lung: frequency and risk factors. BMC Pulm Med. 2012;12:2. doi:10.1186/1471-2466-12-2.
- Glodny B, Schönherr E, Freund MC, et al. Measures to prevent air embolism in transthoracic biopsy of the lung. AJR Am J Roentgenol. 2017;208(5):184-191. doi:10.2214/AJR.16.16048.
- Malik N, Claus PL, Illman JE, et al. Air embolism: diagnosis and management. Future Cardiol. 2017;13(4):365-378. doi:10.2217/fca-2017-0015.
- Blanc P, Boussuges A, Henriette K, Sainty JM, Deleflie M. Iatrogenic cerebral air embolism: importance of an early hyperbaric oxygenation. Intensive Care Med. 2002;28(5):559-563. doi:10.1007/s00134-002-1255-0.
- Ramaswamy R, Narsinh KH, Tuan A, Kinney TB. Systemic air embolism following percutaneous lung biopsy. Semin Intervent Radiol. 2014;31(4):375-377. doi:10.1055/s-0034-1393975.
- Zangan SM, Yu Q. Review of air embolism for the interventional radiologist. Arab J Intervent Radiol. 2024;8:6-12. doi:10.1055/s-0043-1777810.
- Sandoval JI, Das JM. Anterior spinal artery syndrome. In: StatPearls. StatPearls Publishing; 2023.
- Chang HC, Yang MC. Systemic air embolism after percutaneous computed tomography-guided lung biopsy due to a kink in the coaxial biopsy system: a case report. BMC Med Imaging. 2018;18(1):1. doi:10.1186/s12880-018-0245-9.
- Muth CM, Shank ES. Gas embolism. N Engl J Med. 2000;342(7):476-482. doi:10.1056/NEJM200002173420706.
- Hare SS, Gupta A, Goncalves AT, Souza CA, Matzinger F, Seely JM. Systemic arterial air embolism after percutaneous lung biopsy. Clin Radiol. 2011;66(7):589-596. doi:10.1016/j.crad.2011.03.005.
- Rott G, Boecker F. Influenceable and avoidable risk factors for systemic air embolism due to percutaneous CT-guided lung biopsy: patient positioning and coaxial biopsy technique-case report, systematic literature review, and a technical note. Radiol Res Pract. 2014;2014:349062. doi: 10.1155/2014/349062.