
Cancer-Related Pain in Community-Dwelling Older Adults: An Overview of Assessment and Management
Authors: Roma Tickoo, MD, MPH,Paul Glare, MD, Amitabh Gulati, MD, Andreas Rimner, MD, Eric Lis, MD
A Primary Care Perspective on Cancer-Related Pain in Older Adults: Part 1
The older population in 2030 is projected to be twice as large as their counterparts in 2000, growing from 35 million to 72 million and representing nearly 20% of the total US population.1 The aging population is expected to have an impact on cancer burden in the future, with the number of new cancer patients expected to more than double from 1.36 million in 2000 to almost 3.0 million in 2050.2 Among these patients, pain management is an essential component to providing good care for quality of life. Today, effective cancer-related pain management in ambulatory patients dwelling in the community relies on impeccable coordination, communication and delivery of care by multiple disciplines and sub-specialties at tertiary cancer centers. These sub-specialties work closely together or individually in managing cancer-related pain (such as but not limited to a primary oncologist, radiation oncologist, pain management or palliative medicine teams) governed by the presentation of pain and the type of intervention it demands.
_________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
A Guide to Recognizing Common Cancer Pain Syndromes
Palliative Care in Advanced Cancer in Older Adults
_________________________________________________________________________________________________________________________________________________________________
This first of three articles in a series on cancer-related pain management in older community-dwelling adults gives an overview of the prevalence and burden of pain and describes how to assess it. It also outlines selected cancer-related pain syndromes that primary care clinicians should be aware of, as these syndromes may serve as potential triggers for early communication and alert for the primary oncologist and timely triage. The second article in the series will go into further detail about pharmacological management of cancer-related pain in older patients, the role of the clinical pharmacist, and a brief discussion on aberrant drug use. The third and final article will present three case scenarios ultimately showing how the primary care provider can identify, build networks, and partner with locally available sub-specialty referrals. The third article will also synthesize the findings of these three articles into a final summary of recommendations, strategies, and take-home points for the clinician.
Prevalence of Pain in Cancer Patients
The first step in this direction is to understand the phenomenology and assessment of pain. A study by Vuorien3 identified that the prevalence of pain in newly diagnosed cancers is about 28%. More recently, in retrospective cohort study of 505 ambulatory oncology patients followed over nearly 2 years with newly diagnosed stage IV solid tumors at a comprehensive cancer center, Isaac and colleagues4 concluded that while 340 (67.3%) were pain-free at the initial visit, 90 (17.8%) experienced mild pain, 48 (9.5%) experienced moderate pain, and 27 (5.4%) experienced severe pain. In another, the study on pain depression, and fatigue in community-dwelling adults with and without a history of cancer which specifically examined the prevalence of and factors associated with the multiple symptoms in those with a history of cancer, it was empirically reported that community-dwelling adults with a history of cancer had a significantly higher prevalence of these symptoms compared to those without a history of cancer. This was done after controlling for the influence of coexisting medical conditions, sociodemographic and access to care factors. Overall, patients with a history of cancer had a higher prevalence of pain (33% vs 29%; P<.0001), depression (21% vs 18%; P<.0001), and fatigue (25% vs 18%; P<.0001) compared to those without a history of cancer.5
In a study by Cleeland and colleagues6 in 1994, using the World Health Organization guidelines for analgesia, an assessment on the severity of pain during the week preceding the study was made for 1308 outpatients with metastatic cancer from 54 treatments locations affiliated with the Eastern Cooperative Oncology Group. Sixty-seven percent of the patients reported having taken analgesic drugs daily during the week preceding the study, and 36% had pain severe enough to impair their ability to function. Of those with pain, 42% reported having received inadequate analgesic therapy.6 In a cross-sectional cohort study, 24,410 elderly out-patients were assessed for pain and evaluated for factors associated with receiving opioid prescriptions (OP). The proportion of patients with an OP increased as pain score/severity increased: 10% of those with no pain, 24% of those with mild pain, 45% of those with moderate pain, and 67% of those with severe pain. More specifically, for those with severe pain, 41% filled an OP within 7 days of assessment for pain, and 26% had an OP from the 30 days before assessment for pain, leaving 33% without an OP. The authors also concluded that despite a generous time window for capturing OPs, the proportion of patients without an OP seemed high.7
Assessment of Cancer-Related Pain
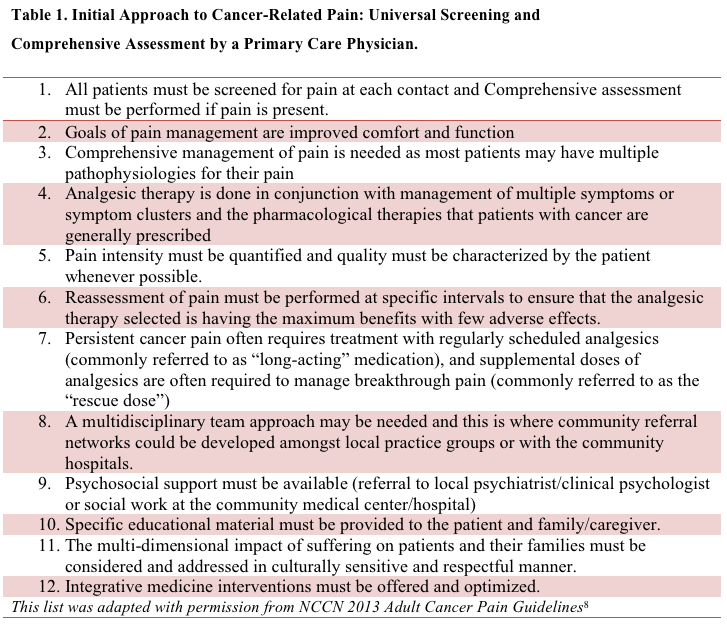
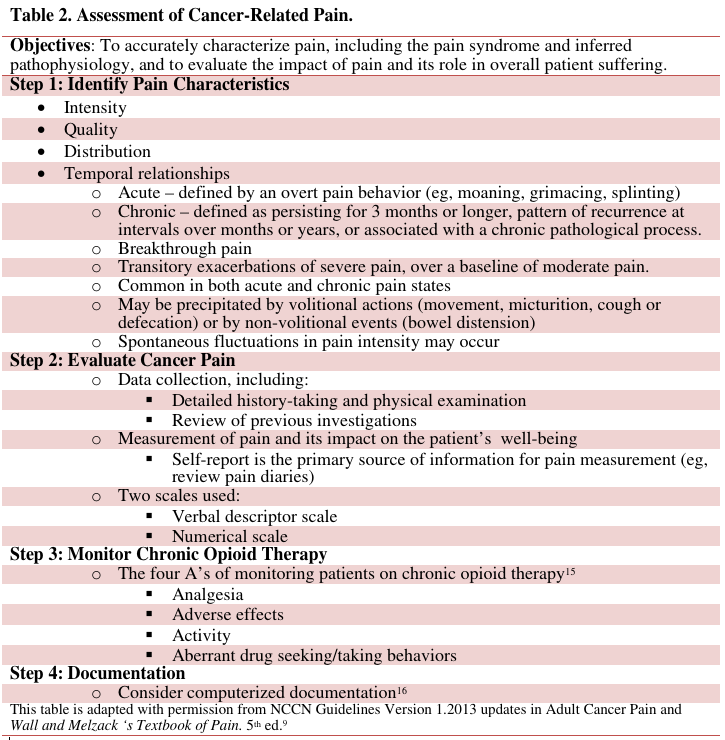
Irrespective of age or setting of care, a comprehensive assessment of the patient is the key to the optimal treatment of cancer pain (Table 18and Table 29). An understanding of the many factors influencing the pain experience is critical to holistic pain management; these factors include pathophysiology (ie, underlying mechanism of pain), cognitive (ie, meaning of the pain), emotional (ie, affective and existential), social (ie, personal history), and environmental factors.While poor assessment has been identified as the principal barrier to effective pain management,10 it must be emphasized that it may take an extended period of time to determine the precise cause of the pain, as more information about the patient and their disease comes to light.11 For example, an older patient with a history of degenerative disc disease and osteoporosis with metastatic bone disease who develops new back pain will require a careful work-up, including magnetic resonance imaging (MRI) of the spine, and may need consultation by an orthopedist, neurosurgeon, radiation oncologist and/or interventional radiologist. Analgesia should not be withheld while the results of the work-up are awaited and a decision about disease-specific therapies is pending.
Ideally, anti-cancer therapies such as surgery, radiation, or chemotherapy are given to eliminate the noxious stimulus and eliminate the cause of the pain. In many older patients, however, the pain may be due to advanced, progressive disease, and the options for treatment may be limited. Interventions may be poorly tolerated and compliance to go through treatment may be impacted due to sub-optimal analgesia. Provision of analgesia thus becomes the initial and main goal of treatment. When permissible by patients’ insurance plans, opportunities for nonpharmacologic and interdisciplinary collaborative approaches and interventions, such as physical therapy, transcutaneous electrical nerve stimulation, cognitive behavioral therapies, acupuncture, and other complementary and alternative therapies must be encouraged. These can be instituted concurrently as medication-sparing modalities of treatment.
The assessment of pain in the older adult presents some unique challenges. Older patients are often reticent to report pain and they are more likely to describe pain as aching, soreness, or discomfort rather than pain per se. This may be because they believe pain is an inevitable part of aging that must be tolerated. Reliable pain measurements may be obtained from older patients, even if they are mildly or moderately cognitively impaired.12 While absence of changes in vital signs or behavior should not be used as sole indicators of pain,13 behavioral observations need to be used such as a decline in their functional status, mood changes leading to depression, increased agitation and confusion, or an altered appetite especially in those who are severely demented. Here, the Pain Assessment and Advanced Dementia Scale can be helpful.14 A home health aide or family member may also be able to provide corroborative pain reports.
Pain scales should be used in the elderly, and they have been shown to increase the diagnosis of pain, especially among patients aged 85 years and older. Patients’ own reporting of pain may, depending on which kind of pain scales they prefer to use. Pain intensity scoring should be attempted verbally first. The FACES Pain Rating Scale while useful should be avoided especially in the cognitively impaired, as they may wrongly identify the facial expressions with their feelings rather than pain.15 Patients with impaired communication due to language barriers, aphasias, cognitive dysfunction, and mechanical ventilation present a challenge for the clinician trying to obtain a comprehensive pain assessment.
(Physical Examination and Conclusion on next page)
Physical Examination
The clinician needs to be familiar with the common cancer pain syndromes (eg, epidural disease, plexopathies in order to facilitate identification of the cause so that treatment can be initiated and morbidity (eg, paraplegia and incontinence due to cord compression) can be prevented or minimized. A complete list of these syndromes is beyond the scope of this review; a selected list of cancer-related pain syndromes are outlined below.16 Knowledge and close attention to what is causing pain will result in early recognition, action, and relief of the patient’s suffering.
- Acute pain syndromes
- Acute pain associated with diagnostic interventions (eg, biopsy-related pain)
- Acute pain associated with therapeutic interventions (eg, postoperative pain, anagelsic techniques, anticancer therapies, chemotherapy toxicity)
- Chronic pain syndromes
- Bone pain (eg, metastic bone disease, vertebral syndromes, skull metastasis)
- Cranial neuralgia (eg, glossopharyngeal, trigeminal)
- Ear and eye pain (eg, otaglia)
- Radiculopathy
- Mononeuropathy
- Peripheral neuropathies
The physical examination should focus on pathologic conditions that are expected to cause pain. The painful area should be carefully examined to determine if palpation or manipulation of the site produces pain. Common sites of pain referral (eg, shoulder pain from subdiaphragmatic lesions) should be kept in mind when performing the examination. The neurological component of the physical examination is emphasized so that syndromes such as vertebral collapse or spinal cord compression are not overlooked.17 Given the clinical implications, at least the basic knowledge and the capability to diagnose such syndromes is essential for every practitioner, even at the community level.
_________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Bilateral Flank Pain in an Older Adult
Chronic Pain Management in the Elderly
_________________________________________________________________________________________________________________________________________________________________
Appropriate diagnostic tests should be performed to determine the cause of pain and extent of disease, and to correlate this information with the findings on the history and physical examination to assure that the appropriate areas of the body have been imaged and the abnormalities found do in fact explain the patient’s pain. As pain may be the harbinger of tumor progression, imaging may need to be repeated. The caveat is that identifying a treatable cause is often relevant in patients amenable to further anti-cancer therapy, so investigations are less appropriate in patients with far advanced cancer on best supportive care or hospice.
Unlike the chronic non-malignant pain population, a physical basis for pain can usually be identified in most cancer patients. However, anxiety, depression and other distress are more common in cancer patients than the general population, so the psychosocial assessment is very important and should emphasize the effect of pain on patients and families, and should address cognitive, meaning of and social aspects of the pain. It is important to identify pathological anxiety or depression that requires specific treatment. Extreme suffering and anguish may present as uncontrollable pain; a “narrative” approach to the cancer pain history will enable the physician to better understand the link between nociception, pain behavior and coping styles, and suffering in the individual patient.11 For example, an older patient who is depressed due to the sudden death of their adult son or daughter could be particularly sad, and psychiatric medications and bereavement counseling may not always be effective for physical pain. Therefore, an assessment to differentiate physical and existential pain must be made.
Follow-up assessment of pain outcomes is also required to evaluate the effectiveness of management, and should document the analgesic effectiveness, improvements in function and mood, adverse effects and any aberrant drug taking behavior. If pain is not well controlled, determine whether the cause is related to the progression of disease, a new cause of pain, or the treatment. The steps for initial assessment should be repeated with each new report of pain as depicted in Table 1.
Conclusion
As the population of those above 65 years increases, it will not be unusual for many of these patients to survive cancers for unforeseen periods of time which may increase their potential as patients and survivors to be suffering with chronic cancer-related pain. It is therefore imperative to view this as a potentially emerging public health issue mandating increased knowledge and enhanced attitudes and practices in management of cancer-related pain in those over the age of 65 years living in the community.
Roma Tickoo, MD, MPH, is an assistant attending in pain and palliative care services, Department of Medicine, at Memorial Sloan Kettering Cancer Center, New York, NY.
Paul Glare, MD, is chief of palliative medicine service, Memorial Sloan Kettering Cancer Center, New York, NY.
Amitabh Gulati, MD, is director of ambulatory pain management, Memorial Sloan Kettering Cancer Center, New York, NY.
Andreas Rimner, MD, is a board-certified radiation oncologist at Memorial Sloan Kettering Cancer Center, New York, NY.
Eric Lis, MD, is director of interventional neuroradiology at Memorial Sloan Kettering Cancer Center, New York, NY.
References
1. Population: Indicator 1. In: Federal Interagency Forum on Aging-Related Statistics. Older Americans 2012: Key Indicators of Well-Being. Washington, DC: US Government Printing Office; 2012:22.
2. Hayat MJ, Howlader N, Reichman ME, Edwards BK. Cancer statistics, trends, and multiple primary cancer analyses from the Surveillance, Epidemiology, and End Results (SEER) Program. Oncologist. 2007;12(1):20-37.
3. Vuorinen E. Pain as an early symptom in cancer. Clin J Pain.1993;9(4):272-278.
4. Isaac T, Stuver SO, Davis RB, et al. Incidence of severe pain in newly diagnosed ambulatory patients with stage IV cancer. Pain Res Manag. 2012;17(5):347-352.
5. Reyes-Gibby CC, Aday LA, Anderson KO, Mendoza TR, Cleeland CS. Pain, depression, and fatigue in community-dwelling adults with and without a history of cancer. J Pain Symptom Manage. 2006;32(2):118-128.
6. Cleeland C, Gonin R, Hatfield AK, et al. Pain and its treatment in outpatients with metastatic cancer. N Engl J Med. 1994;330(9):592-596.
7. Barbera L, Seow H, Husain A, et al. Opioid prescription after pain assessment: a population-based cohort of elderly patients with cancer. J Clin Oncol. 2012;30(10):1095-1099.
8. National Comprehensive Cancer Network. CCN guidelines for treatment of adult cancer pain. www.nccn.org/professionals/physician_gls/pdf/pain.pdf. Accessed November 24, 2014.
9. Cherny N. Assessment of cancer pain in Wall and Melzack's Textbook of Pain. In: Koltzenburg Ma, ed. Assessment of Cancer Pain. 5th ed. Churchill Livingstone; 2006.
10. Von Roenn J, Cleeland, CS, Gonin R, Hatfield AK, Pandya KJ. Physician attitudes and practice in cancer pain management. A survey from the Eastern Cooperative Oncology Group. Ann Intern Med. 1993;119(2):121-126.
11. Lickiss JN. Approaching cancer pain relief. Eur J Pain. 2001;(5 suppl A):5-14.
12. Herr K, Coyne PJ, Key T, et al; American Society for Pain Management Nursing. Pain assessment in the nonverbal patient: position statement with clinical practice recommendations. Pain Manag Nurs. 2006;7(2):44-52.
13. Beyer J, McGrath PJ, Berde CB. Discordance between self-report and behavorial pain measures in children aged 3-7 years after surgery. J Pain Symptom Manage. 1990;5(6):350-356.
14. Warden V, Hurley AC, Volicer L. Development and psychometric evaluation of the Pain Assessment in Advanced Dementia (PAINAD) scale. J Am Med Dir Assoc. 2003;4(1):9-15.
15. Jacox A, Carr DB, Payne R, et al. Management of Cancer Pain. Clinical Practice Guideline Number 9. Rockville, MD: Agency for Health Care Policy and Research, US Department of Health and Human Services, Public Health Service; March 1994. AHCPR Publication No. 94-0592.
16. Portenoy RK, Dhingra LK. Overview of cancer pain syndromes. UpToDate. http://www.uptodate.com/contents/overview-of-cancer-pain-syndromes. Accessed April 10, 2014.
17. Elliott K, Foley K. Neurologic pain syndromes in patients with cancer. Neurol Clin. 1989;7(2):333-360.