
A Practical Approach to Evaluating and Managing Migraines
Gaining your patient’s trust is imperative for the treatment of headaches.
This, along with the etiology of migraine headaches and a discussion of treatment options, was the topic at this afternoon’s session presented by Cindy Cooke, DNP, FNP-C, FAANP, who is adjunct faculty at the University of Mary Bismarck in North Dakota.
The session started with an overview of migraine headaches, including symptoms, primary type headaches, and methods for diagnosing the type of headache.
“Frequency, intensity, duration – these are things that are very important in evaluating patients with headache,” she said.
Headache Diagnosis
She went on to discuss predictors of migraine, which include female gender, aura, high pain severity, disability during headache, photophobia and phonophobia. When seeing a patient with headache, you should conduct a physical (head and neck) exam, as well as a neurological exam, including mental state, cranial nerve function, nuchal rigidity, focal neurological deficits, and coordination and gait.
Next, she discussed the diagnostic criteria for various types of headache, including migraine without aura (Figure 1) and with aura (Figure 2).
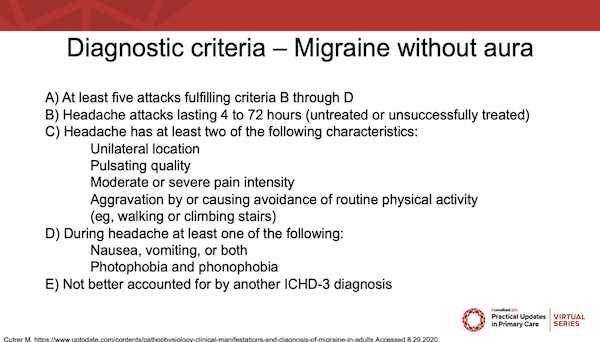
Figure 1.
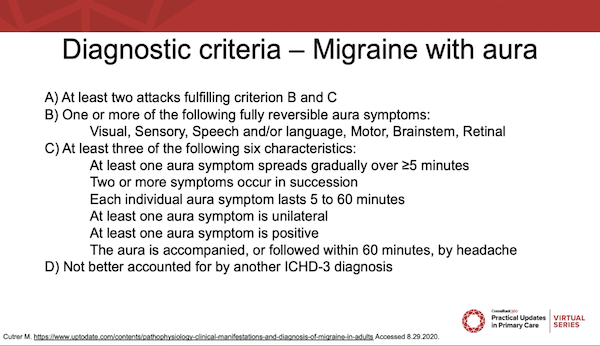
Figure 2.
“There are many things that can trigger migraines, and it is interesting to hear, when people keep a headache diary, what is contributing to it.”
Emotional stress, she said, is the number 1 cause of migraine, followed by odors, hormones, not eating, sleep disturbances, and the weather. Among women, menstruation is also a common trigger of migraine, with 60%-70% of women with migraines experiencing them in association with menses.
Treatment of Migraine
The goal of treatment, she said, is to abort the symptoms as quickly as possible. She suggested that clinicians should start simply—often patients have already tried several over-the-counter remedies. Treatment of nausea and vomiting can help to calm the migraine as well. Pharmacologic treatments (Figure 3) should be started as soon as symptoms appear and are often more effective in a single large dose rather than several smaller doses.
Next, she discussed prevention of migraines, including common therapy options (beta blockers, antidepressants, and anticonvulsants), as well as Botox injections in patients 15 days or more each month. Drugs, she recommended, should be started at a low dose and gradually titrated until benefits are seen or max dose is reached.
Lastly, she stressed the importance of asking patients about medication overuse, a major cause of chronic headaches.
“You need to ask. Be specific in your questions. How much are you taking? How often are you taking medications?”
—Michael Potts
Reference:
Cooke C. A Practical Approach to Evaluating and Managing Migraines. Talk presented at: Practical Updates in Primary Care 2020 Virtual Series; October 9-10, 2020; virtual.