
Diagnosing Arthralgias in Primary Care
Evaluating and diagnosing arthralgias can be challenging, especially when patients present with similar symptoms. In his session this afternoon, Patrick Astourian, MSPA-C, talked about differentiating between inflammatory and noninflammatory arthritis, understanding what diagnostic tests to order on the swollen joint, and when to refer your patient for consultation.
Patrick is a physician assistant in rheumatology at the Arthritis Care and Research Center in San Diego, California.
Differentials, Diagnostic Tests, and Referrals
Infection
Patrick recommends ruling out infection first. For patients who present with hot, swollen joints, the recommended ancillary tests include complete blood count, CHEM 14, uric acid, and C-reactive protein.
Patrick also recommends aspirating the joint to evaluate the fluid. If the fluid appears cloudy, send it out for stat analysis. If the analysis confirms an infection, start treatment with antibiotics.
“Consider intravenous antibiotics if the patient is febrile or if there is evidence of septicemia,” Patrick said. “Also make sure to get culture and sensitivity to make sure the bug is sensitive to the antibiotic.”
Inflammatory arthritis
Order routing laboratory tests and an x-ray. Results are normal except for elevated erythrocyte sedimentation rate and C-reactive protein levels. After ruling out infection, you can consider inflammatory arthritis if the patient does not have a history of traumatic onset of joint pain or swelling.
Patrick recommends ordering a baseline rheumatology panel, including rheumatoid factor, cyclic citrullinated peptide, antinuclear antibodies with reflex, uric acid, and human leukocyte antigen B27. If any of these values come back elevated, refer your patient to a rheumatologist for a consultation. Also remember to send copies of your patient’s laboratory results and x-ray reports.
Rheumatoid arthritis
Rheumatoid arthritis is a symmetrical inflammatory arthritis, according to Patrick. Patients typically present with positive rheumatoid factor and cyclic citrullinated peptide results, as well as pain and swelling in the wrists and small joints of the hand and feet. Results of an x-ray will show erosions on the hand or foot.
Treatments for rheumatoid arthritis can stop joint pain and swelling
Early treatment will give better long-term results.
“You don’t want to wait to refer to rheumatology, because the longer you wait, the more damage is going to be permanent to the joints is being done,” Patrick said.
Systemic lupus erythematosus
Lupus is a chronic disease that causes systemic inflammation that can affect multiple organs, including the kidneys and/or brain. Patients commonly present with malar rash, oral ulcers, alopecia, fatigue, asymmetrical joint swelling, and photosensitivity.
About 20% of patients with lupus are children, and women are 10 times as likely than men to have lupus.
“Treatment of lupus depends on the organs involved, but hydroxychloroquine is typically prescribed,” Patrick said.
Spondyloarthropathies
The 2 most common spondyloarthropathies are psoriatic arthritis and ankylosing spondylitis. In these patients, human leukocyte antigen B27 and C-reactive protein levels are typically elevated, and the large joints particularly in the lower extremities, distal joints of the fingers and toes, and the back and sacroiliac joints of the pelvis are often involved. Nail pitting is also common.
“Remember that the typical patient goes 7 to 8 years and will see at least 5 providers before being diagnosed,” Patrick said.
Men are more likely than women to have ankylosing spondylitis, and Patrick said that about 20% of patients with psoriasis will develop psoriatic arthritis.
Crystalline arthritis
Calcium pyrophosphate dihydrate crystal deposition disease (CPPD) and gout need to be ruled out before making a diagnosis of crystalline arthritis. To do so, send the aspirated fluid for a crystal analysis under a polarized microscope. Calcium urate crystals can be seen on x-ray, and uric acid crystals can be seen on synovial analysis.
Patrick said that serum uric acid can be normal during an acute gout attack and that uric acid levels should be rechecked 4 weeks after the acute attack. Treatment includes naproxen or a methylprednisolone dose pack.
Osteoarthritis
X-ray results are key for making a diagnosis. Points to observe include the meniscus in the knee and any presence of osteophytes. For patients with severe osteoarthritis who do not have meniscus visible and have multiple osteocytes, referral to an orthopedist is recommended. See Figure 1 for a list of treatments (click the image to enlarge).
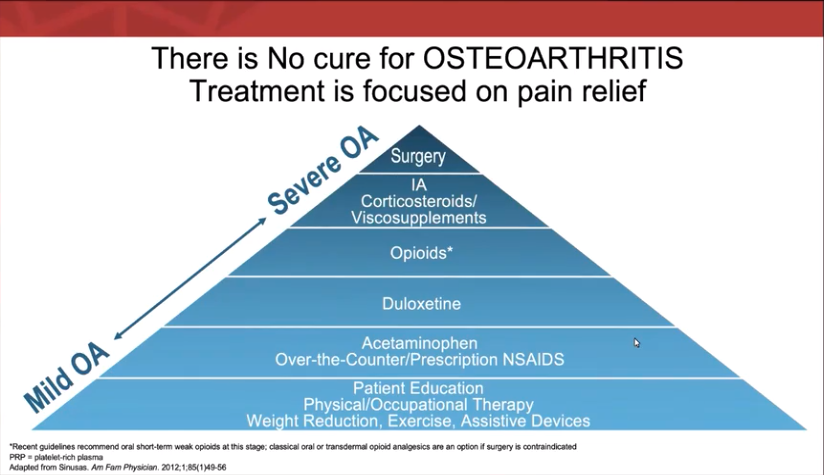
“If they fail all these treatments, refer the patient to orthopedics for consultation and possible knee replacement,” Patrick said.
—Amanda Balbi
Reference:
Astourian P. Evaluation and management of patients with arthralgias. Talk presented at: Practical Updates in Primary Care 2020; December 4-5, 2020; Virtual.