
Peer Reviewed
What Is the Cause of This Infant’s Cough and Rhinorrhea?
A 6-month-old girl with a history of an H-type tracheoesophageal fistula (TEF) that had been repaired at 2 weeks of age presented to the pediatrician’s office. The girl had had a 1-week history of cough and rhinorrhea, and the cough had not been associated with feeding, position, hemoptysis, or sputum production.
On physical examination, the infant was afebrile, with normal vital signs and an oxygen saturation greater than 95% on room air. She was well appearing and slightly tachypnic but not in any respiratory distress, with unremarkable lung examination findings on auscultation and a respiratory rate of 56 breaths/min.

Results of a chest radiograph obtained in the pediatrician’s office were significant for alveolar infiltrates (Figures 1 and 2), and the patient was referred to a pediatric pulmonologist.
What is causing the alveolar infiltrates visible on radiographs?
Answer: Barium aspiration

The chest radiograph results suggested disease in the alveolar space as evidenced by alveolar infiltrates. Substances that may accumulate in the alveolar space include surfactants, calcium, hemosiderin, and radiopaque substances such as barium.
The diagnosis became evident after a review of our patient’s hospitalization history. She initially had presented in the first 2 weeks of life with failure to thrive and feeding intolerance. A barium swallow was done at that time, resulting in barium aspiration and chemical pneumonitis requiring intensive care.
A chest radiograph that was taken immediately after the barium aspiration is shown in Figure 3. Later, a more specific contrast study revealed the H-type TEF. Over the following 2 weeks, the patient recovered from her pneumonitis and subsequently underwent a successful TEF repair.
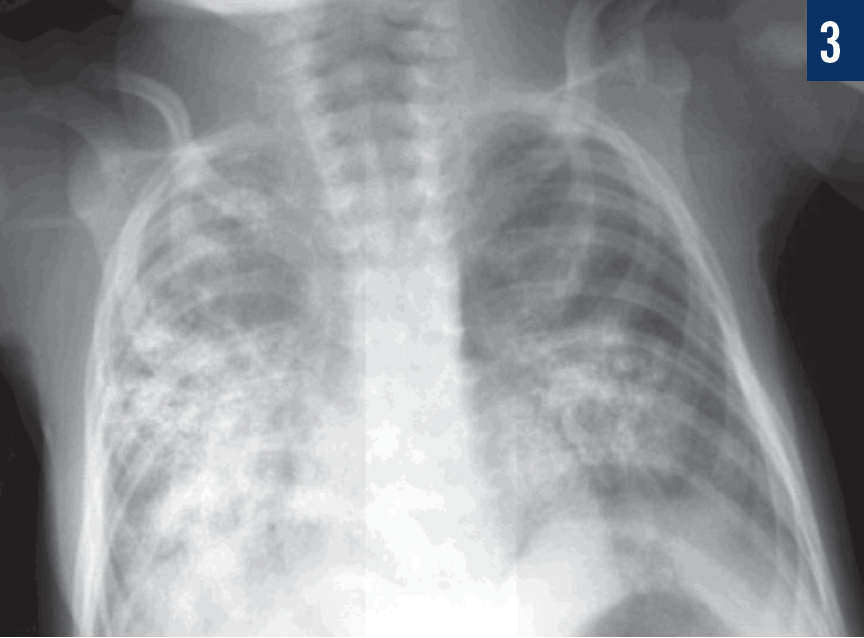
A radiograph ordered by the pediatrician when the girl presented at age 6 months (Figures 1 and 2) showed residual barium from the initial insult and actually demonstrated an improvement compared with findings from the radiographs that had been taken immediately after aspiration (Figure 3).
DIFFERENTIAL DIAGNOSIS
Barium aspiration should be considered if a patient’s history includes a barium study, even if the study was not recent. Barium is an inert chemical with a high molecular weight that gives dramatic evidence of its presence on radiographs, but it is generally benign when introduced to the respiratory system.1 When a small amount of barium is aspirated in the tracheobronchial tree, it is rapidly cleared by coughing or mucociliary clearance. However, if a significant amount of barium is aspirated, it may be retained in the interstitium or phagocytized by macrophages, leading to prolonged retention for months to years.1
If thorough history-taking does not divulge the diagnosis in a patient with alveolar infiltrates on chest radiograph, the next best step in evaluation is referral to a pediatric pulmonologist for high-resolution computed tomography and bronchoscopy with bronchioalveolar lavage.
Another possibility to consider in the differential diagnosis is pulmonary alveolar proteinosis (PAP), which is a problem with surfactant homeostasis and is characterized by the accumulation of lipoproteinaceous material in the alveoli and inside alveolar macrophages.2 The major defect in this condition is the inability of macrophages to be activated by cytokine granulocyte-macrophage colony-stimulating factor (GM-CSF).3 Without appropriate stimulation by GM-CSF, macrophages internalize but do not catabolize surfactant.3
PAP may be the result of a genetic defect, an acquired autoimmune disease, or the result of a toxic exposure such as to chemotherapy.2 The presentation of PAP is variable, and it can present as respiratory failure in infancy or as slowly progressive dyspnea, depending on the underlying defect.2,3 Bronchioalveolar lavage in these patients reveals a milky brown fluid that is positive on periodic acid–Schiff staining with foamy, surfactant-laden alveolar macrophages.2,3
The differential diagnosis should also include pulmonary alveolar microlithiasis (PAM), a rare autosomal recessive mutation affecting the alveolar phosphate cotransporter.4 When this transporter is defective, phosphate builds up in the alveolar space, yielding microliths.4 Although the classic presentation of PAM is an abnormal chest radiograph in an asymptomatic patient, the natural history of this disease is progressive end-stage lung disease.4 Bronchioalveolar lavage or biopsy can confirm the diagnosis by revealing the calcified spherules.4
Diffuse alveolar hemorrhage (DAH) is another potential differential diagnosis. DAH can be caused by a large group of diseases in which there is capillary hemorrhage into the alveolar space.5 It is typically caused by an immune-mediated process of vasculitis or capillaritis such as Goodpasture syndrome, but it also may be the result of a nonimmune process, a toxin, a drug-mediated reaction, or an idiopathic process (idiopathic pulmonary hemosiderosis).5,6 DAH is evidenced by hemosiderin-laden macrophages in bronchoalveolar lavage fluid.5 Consideration of infectious causes of diffuse alveolar infiltrates, such as Pneumocystis jirovecii, may be necessary if suggested by the patient’s history or immune status.
Potential Complications of Barium
Barium provides a seemingly ideal modality for evaluating the swallowing mechanism, but cases of serious pathology and even death have been reported secondary to massive barium aspiration.7,8 The pathophysiology of these severe consequences is likely 2-fold, secondary to mechanical obstruction leading to alveolar dead space, and to an acute inflammatory reaction related to the aspiration of erosive gastric contents in addition to barium.9 Despite this risk, adverse events are extremely rare, and barium contrast studies should not be avoided because of this potential complication.1
Long-term complications of retained barium in the alveolar space after aspiration are somewhat controversial. Voloudaki and colleagues9 reported the presence of interstitial fibrosis in an adult patient 1 year after barium aspiration. However, contrast bronchography had been commonly used in the past without consequence, and baritosis is widely accepted as a benign pneumoconiosis that self-resolves in time once the exposure to barium is removed.10,11
The Take-Home Message
Barium aspiration is typically a benign complication of contrast diagnostic evaluation. In rare cases, severe, life-threatening chemical pneumonitis can occur if the aspiration is large. Alveolarized barium can persist for months to years and will be visualized on radiograph as diffuse alveolar opacities.
Our patient recovered easily from her viral upper respiratory infection. The aspirated barium currently is not causing our patient any significant disease, and she continues to be asymptomatic. The plan is to monitor her with serial imaging every 6 months for resolution of the alveolarized barium.
Jennifer Bouso, MD, MSPH, is a resident in the University of Florida Pediatrics Residency Program at Sacred Heart Hospital in Pensacola, Florida.
Okan Elidemir, MD, is a pulmonologist in the Department of Pediatric Pulmonology at Nemours Children’s Specialty Care in Pensacola, Florida.
REFERENCES:
- Skucas J. Imaging contrast agents and pharmacoradiology. In: Gore RM, Levine MS, eds. Textbook of Gastrointestinal Radiology. Vol 1. 4th ed. Philadelphia, PA: Elsevier Saunders; 2015:3-22.
- Trapnell BC, Whitsett JA, Nakata K. Pulmonary alveolar proteinosis. N Engl J Med. 2003;349(26):2527-2539.
- Suzuki T, Sakagami T, Young LR, et al. Hereditary pulmonary alveolar proteinosis: pathogenesis, presentation, diagnosis, and therapy. Am J Respir Crit Care Med. 2010;182(10):1292-1304.
- Homer RJ. Depositional diseases of the lungs. In: Grippi MA, Elias JA, Fishman JA, Kotloff RM, Pack AI, Senior RM, eds. Fishman’s Pulmonary Diseases and Disorders. Vol 1. 5th ed. New York, NY: McGraw-Hill; 2015:945-955.
- Ioachimescu OC, Stoller JK. Diffuse alveolar hemorrhage: diagnosing it and finding the cause. Cleve Clin J Med. 2008;75(4):258-265.
- Zucker EJ, Guillerman RP, Fishman MP, Casey AM, Lillehei CW, Lee EY. Diffuse lung disease. In: Coley BD, ed. Caffey’s Pediatric Diagnostic Imaging. 12th ed. Philadelphia, PA: Elsevier Saunders; 2013:594-601.
- Zhang L, Yang Y, Zhang J, Zhou X, Dong H, Zhou Y. Barium sulfate aspiration: severe chemical pneumonia induced by a massive reflux of contrast medium during small bowel barium enema. Forensic Sci Int. 2015;253:e16-e19.
- Jackson M, Kapur N, Goyal V, et al. Barium aspiration in an infant: a case report and review of management. Front Pediatr. 2014;2:37. doi:10.3389/fped.2014.00037.
- Voloudaki A, Ergazakis N, Gourtsoyiannis N. Late changes in barium sulfate aspiration: HRCT features. Eur Radiol. 2003;13(9):2226-2229.
- Hundemer GL, Kumar V, Vaduganathan M. Large-volume barium aspiration. Proc (Bayl Univ Med Cent). 2015;28(2):183-184.
- Doig AT. Baritosis: a benign pneumoconiosis. Thorax. 1976;31(1):30-39.