
Peer Reviewed
Sore Throat After Ingestion of an Unknown Substance
Introduction. A 34-year-old unhoused man with a history of polysubstance abuse presented to the emergency department with a sore throat for the past 4 days.
History. The patient stated that he was in significant pain and felt dehydrated due to his inability to eat. He said 4 days prior to his presentation, he found a small bag with powder in the street that contained a crystalline substance, which would easily break apart in his hand if crushed. Believing it to be methamphetamine, he ingested the substance. After ingestion, he immediately experienced a burning sensation inside his mouth and down his throat, radiating into his neck. Since that time, he has been unable to eat or drink due to the pain. He did not have chest pain, shortness of breath, abdominal pain, nausea, hemoptysis, or hematemesis.
The patient’s physical examination revealed an agitated, well-developed man with normal vital signs. His oropharyngeal examination showed an ulcer on the right anterior tonsillar pillar as well as erythematous tonsils of normal size. He had poor dentition and dry mucous membranes. His heart had a regular rate and rhythm. Lungs were clear to auscultation bilaterally. There was no crepitus to palpation of the neck or chest wall, although he did have tenderness over the bilateral sternocleidomastoid muscles. His abdomen was soft and non-tender with present bowel sounds. There were skin changes consistent with intravenous (IV) drug usage on his left arm.
Diagnostic testing. The patient’s white cell count was 12.04 (normal range, 3.50-10.80) and his creatinine was 2.70 (normal range, 0.7-1.2). Although no alcohol was detected in his blood sample, a drug screening was positive for amphetamines and cannabinoids. His respiratory viral panel was negative, and his rapid step was positive. The oral ulcer was cultured as well. Due to his trouble swallowing, a chest x-ray was obtained (Figure 1), which showed pneumomediastinum. The patient’s chest and neck computed tomography (CT) showed moderate pneumomediastinum (Figure 2) and extensive subcutaneous emphysema within the base of the neck (Figure 3).
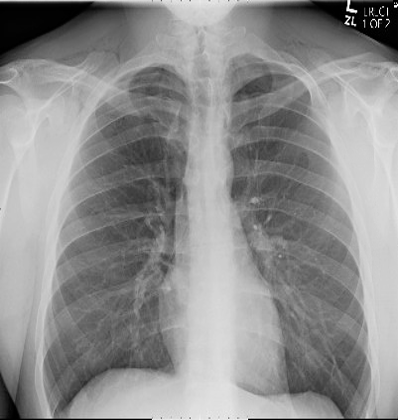
Fig. 1. The patient’s anteroposterior chest x-ray is shown.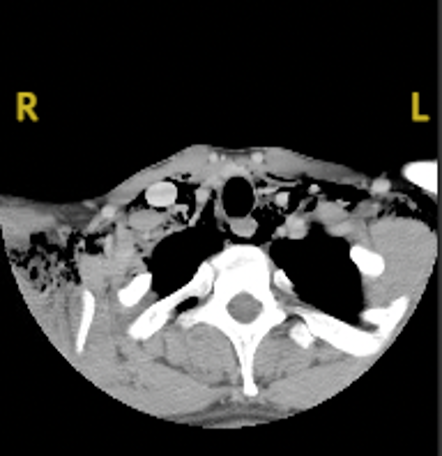
Fig. 2. The patient’s neck CT with contrast is shown.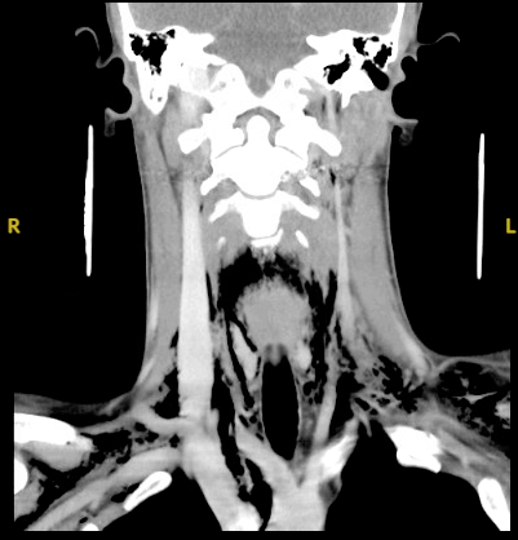
Fig. 3. The patient’s soft tissue neck CT with contrast is shown.