
Peer Reviewed
A Challenging Case of Recalcitrant Facial and Disseminated Rash in a Patient with Autoimmune Comorbidities
Introduction. A 35-year-old woman with systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), chronic urticaria, asthma, Hashimoto thyroiditis, and recurring seizures presented to dermatology with a 3-month rash.
History. The scaly, erythematous rash started on her abdomen and spread to her shins, groin, wrists, arms, and face. Previous treatments with clobetasol, hydrocortisone, 0.025% triamcinolone, and clotrimazole reduced itching but failed to clear the rash.
She was recently hospitalized for a seizure and discharged on lamotrigine extended release 200 mg two times a day (BID) and levetiracetam 1000 mg BID for maintenance therapy. Recent laboratory examinations show normal C3, C4, and anti-dsDNA, with positive anticardiolipin antibody, beta-2 glycoprotein, and lupus anticoagulant. The patient has a history of pregnancy loss and pulmonary embolism and is on warfarin. She lives with a cat that has been ill recently from a skin infection. Her medical history includes hydroxychloroquine treatment for SLE and APS. The patient was a fall risk because of her recent seizures.

Figure 1. The patient presented with a rash that started on her abdomen, but spread to her face as well as her shins, groin, wrists, and arms.
Figure 2. The rash was present on both wrists.The patient’s physical examination reveals erythematous, scaly, well-demarcated plaques involving the forehead, bilateral eyebrows (hair follicles), nasal bridge, and periorbital regions (Figure 1). The distribution appears to spare the nasolabial folds. There is mild desquamation noted within the affected areas, and no signs of ulceration, crusting, or pustules are evident. The rash is symmetrically distributed. The rash is also present on her groin, legs, wrist (Figure 2), and abdomen (Figure 3).

Figure 3. A rash can be seen on lhe patient's lower abdominal fold.Diagnostic Testing. Skin biopsy was performed on patient’s abdomen and wrist. Further diagnostic testing included a potassium hydroxide (KOH) stain (Figure 4).
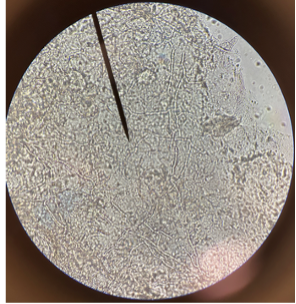
Figure 4. Diagnostic testing included a potassium hydroxide (KOH) stain