
Peer Reviewed
When Adequate Sampling and Communication between Clinicians and Pathologists Matter: A Case of Cutaneous Sarcoidosis Mimicking Squamous Cell Carcinoma
Introduction. A 60-year-old woman presented for Mohs micrographic surgery to remove a suspected squamous cell carcinoma on the right nasal sidewall.
History: The patient had a history of multiple basal cell carcinomas and SCCs, as well as of pulmonary and ocular sarcoidosis. The lesion appeared as a reddish-brown indurated plaque distorting the right nasal sidewall and distal nose with irregular thickening (Figure 1), and previous biopsy (performed in general dermatology clinic) was read as well differentiated SCC with surrounding granulomatous inflammation.

Figure 1. Reddish-brown indurated plaque encompassing the right nasal sidewall and distal nose.
Diagnostic testing. Given the lack of typical features of SCC such as well-demarcated borders and ulceration as well as the patient’s history of sarcoidosis, a repeat biopsy was performed in Moh’s clinic. Histopathology demonstrated more overt pseudocarcinomatous hyperplasia (PCH) with noncaseating granulomas (Figure 2).
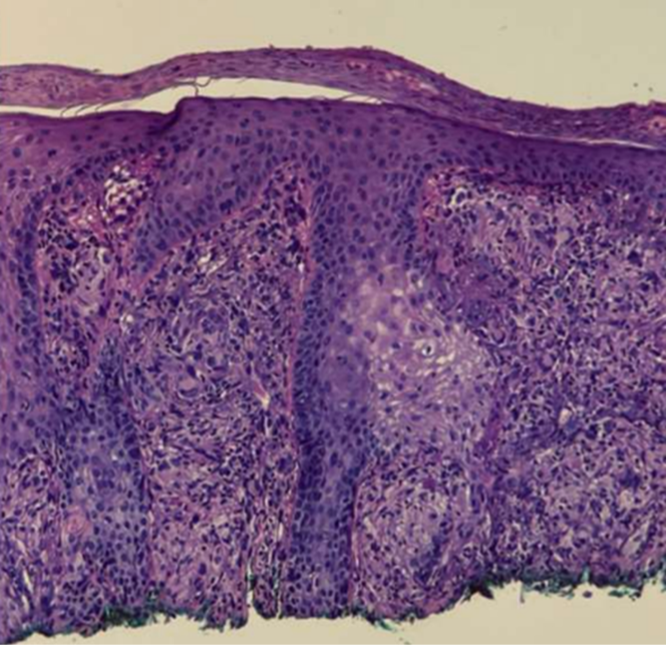
Figure 2. Biopsy of right nasal lesion demonstrating pseudocarcinomatous hyperplasia with noncaseating granulomas.
Differential diagnosis: The presentation of an indurated, verrucous plaque on the nasal sidewall with PCH and granulomatous inflammation prompted consideration of two main diagnoses: verrucous SCC with reactive granulomas and sarcoidosis‐associated epithelial hyperplasia.
Although the epidermal hyperplasia and induration initially suggested verrucous SCC, key histologic features of malignancy, including keratin pearl formation, significant cytologic atypia, frequent mitoses, and stromal invasion, were absent. Clinically, the lesion lacked well-demarcated borders, ulceration, and the rapid growth, pain, or bleeding typical of aggressive keratinocytic neoplasms. Instead, repeat biopsy revealed well-formed, noncaseating granulomas intimately associated with PCH. Negative special stains and cultures excluded atypical mycobacterial and deep fungal infections, and no polarizable material was seen to indicate a foreign-body reaction.
Considering these findings, and given the patient’s known systemic sarcoidosis, the final diagnosis was cutaneous sarcoidosis mimicking SCC, rather than true squamous malignancy.
Treatment and management. The patient was initially started on both hydroxychloroquine 400mg once daily as well as systemic methotrexate 15mg each week after pulmonology evaluation for sarcoidosis involving other organs. However, she developed significant gastrointestinal side effects of methotrexate after a few weeks and was unable to tolerate continued therapy. Hydroxychloroquine was well tolerated over the ensuing months and chosen for its efficacy in cutaneous sarcoidosis.
Outcome and follow up. Over the ensuing months on hydroxychloroquine, the nasal plaque showed marked reduction in induration and erythema, with near-complete clinical resolution. The patient continues hydroxychloroquine with routine ophthalmologic and laboratory monitoring as well as regular dermatology and pulmonology follow-up and reports no adverse effects.
Discussion. Cutaneous sarcoidosis is a granulomatous skin disorder with diverse clinical and histopathological presentations. Common variants include maculopapular, nodular, lupus pernio, and plaque-type sarcoidosis. The histological finding PCH, a benign reactive proliferation of the epidermis, can mimic SCC, particularly when associated with granulomatous inflammation.1
Here, we report a “near-miss” case of cutaneous sarcoidosis presenting as a nasal lesion initially misdiagnosed as SCC, highlighting the diagnostic challenges of PCH and the importance of clinical-pathological correlation.
Cutaneous sarcoidosis remains a diagnostic challenge due to its variable clinical and histopathological presentations. The gross appearance of an individual lesion may resemble SCC due to its indurated appearance, architectural distortion and frequent involvement of the head and neck. However, distinguishing features of lupus pernio, characterized by violaceous, indurated plaques typically affecting the nose, cheeks, ears, and lips, can provide critical diagnostic clues. The reddish-brown coloration and lack of ulceration further aid in differentiation. The patient’s medical history and risk factors are also important factors in differentiating sarcoidosis from SCC.
SCC and cutaneous sarcoidosis may have overlapping histologic features, as illustrated by this case. PCH presents as a benign, reactive epidermal proliferation which can be commonly mistaken for SCC.1 The differentiation between PCH and SCC hinges on the absence of cellular atypia in PCH, which can be triggered by a variety of inflammatory and infectious conditions such as sarcoidosis, deep fungal infections, tuberculosis, and hypertrophic lichen planus. Specifically in this case, we discuss the association between sarcoidosis and PCH, which has been infrequently reported in the literature, primarily in the setting of verrucous sarcoidosis.1,2
An additional histological factor, which made this case more diagnostically challenging was the granulomatous inflammation. While non-caseating granulomas are a hallmark of sarcoidosis, granulomatous inflammation can also occur as a reactive process in SCC, potentially leading to diagnostic confusion. This overlap is particularly problematic when tissue sampling is limited or inadequate for thorough histological evaluation. Moreover, granulomas may induce PCH, possibly due to pro-inflammatory cytokines such as tumor necrosis factor-alpha and interferon-gamma, which drive epidermal proliferation.3,4
Immunohistochemical staining for p53, matrix metalloproteinase 1, and E-cadherin may aid in differentiating PCH and SCC.1 Specifically, p53 and MMP-1 staining is diffusely reactive in the nuclei of invasive tumor cells while reactivity to p53 and MMP-1 is only seen in the nuclei of cells in the basal layer in PCH In contrast, E-cadherin staining is significantly decreased in SCC compared to PCH.1 Additionally, a multiplex qRT-PCR assay targeting the genes C15orf48 and KRT9, has shown high accuracy in distinguishing SCC from PCH, though this is still investigational and not routinely used in medical practice.5
This case highlights how heightened vigilance with adequate sampling and minimal atypicality is key to the right differential when evaluating lesions, particularly in patients with known systemic diseases such as sarcoidosis, the great imitator.
AUTHORS
Catherine E. Lyons, BS, BA1; Aaron D. Smith, BS1; Nicole L Edmonds, MD2; Anya S. Chan3; Vandana Nanda, MD3; Margaret Noland, MD2; R Hal Flowers, MD2
AFFILIATIONS
1University of Virginia School of Medicine
2Department of Dermatology, University of Virginia School of Medicine
3Advanced Dermatology of Charlottesville
CITATION
Lyons CE, Smith AD, Edmonds NL, et al. When adequate sampling and communication between clinicians and pathologists matter: a case of cutaneous sarcoidosis mimicking squamous cell carcinoma. Consultant. 2025;65:1. DOI: 10.25270/con.2026.01.000001
DISCLOSURE
The authors report no relevant financial relationships.
The authors obtained written consent from patients for their photographs and medical information to be published in print and online and with the understanding that this information may be publicly available. Patient consent forms were not provided to the journal but are retained by the authors.
ACKNOWLEDGMENTS
None.
CORRESPONDENCE
Catherine Lyons, BS, BA, 1221 Lee St 3rd Floor, Charlottesville, VA 22903 (Email: vss7ua@virginia.edu)
References
- Zarovnaya E, Black C. Distinguishing pseudoepitheliomatous hyperplasia from squamous cell carcinoma in mucosal biopsy specimens from the head and neck. Archives of Pathology & Laboratory Medicine. 2005;129(8):1032-1036. doi:10.5858/2005-129-1032-DPHFSC.
- Sussman ME, Pousti BT, Grossman SK, Lee JB, Hsu S. Verrucous sarcoidosis: a rare clinical presentation of sarcoidosis. Cureus. 2021;13(5):e15175. doi:10.7759/cureus.15175
- Bergeron A, Bonay M, Kambouchner M, et al. Cytokine patterns in tuberculous and sarcoid granulomas: correlations with histopathologic features of the granulomatous response. J Immunol. 1997;159(6):3034-3043.
- Judson MA, Marchell RM, Mascelli M, et al. Molecular profiling and gene expression analysis in cutaneous sarcoidosis: the role of interleukin-12, interleukin-23, and the T-helper 17 pathway. J Am Acad Dermatol. 2012;66(6):901-910.e9102. doi:10.1016/j.jaad.2011.06.017
- Su A, Ra S, Li X, Zhou J, Binder S. Differentiating cutaneous squamous cell carcinoma and pseudoepitheliomatous hyperplasia by multiplex qRT-PCR. Modern Pathology. 2013;26(11):1433-7. doi:10.1038/modpathol.2013.82.
©2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Consultant360 or HMP Global, their employees, and affiliates.