
Peer Reviewed
Skull Base Tumor Presenting in a 10-Year-Old Girl with Cough
Introduction. A 10-year-old girl with a history of allergies and recurrent upper respiratory infections presented to an outpatient pediatric clinic for evaluation of a 3-month dry cough.
History. Previously, providers treated her symptoms with antihistamines, guaifenesin, and macrolide antibiotic courses for secondary infections. Cold beverages or exposure to hot air outdoors worsened the cough. She reported headaches occurring on alternate days, lasting for 10-20 minutes, and resolving without medication. She denied activity or appetite changes, fatigue, fever, congestion, postnasal drip, rhinorrhea, sore throat, blurry vision, vomiting, or urinary changes. On physical examination, her blood pressure was 104/76 and she had otherwise findings within normal ranges. Her linear growth rate was also within normal range.
Diagnostic Testing. Due to the chronicity of the cough, a workup was initiated to evaluate for lower and upper respiratory disease, using a chest X-ray, spirometry, and a standard sinus computed tomography (CT) of the sinuses without contrast. While the chest X-ray and spirometry showed no abnormalities, the CT revealed a large, partially calcified sellar and suprasellar mass measuring at 4 cm (Figure 1). Other than mucosal thickening along both maxillary antral floors, the remainder of the sinus CT was unremarkable.
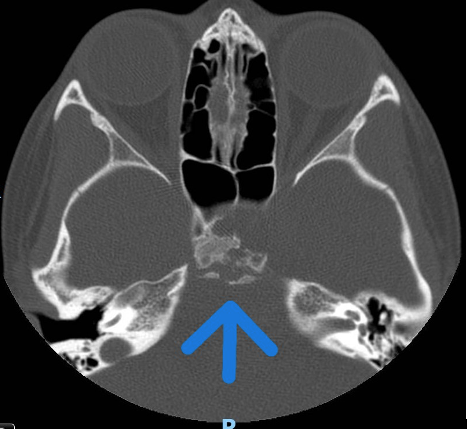
Figure 1. Initial computerized tomography. The maxillary sinus imaging revealed a suprasellar mass (arrow) is shown.
The subsequent brain magnetic resonance imaging (MRI) revealed a heterogeneous mixed cystic and solid sellar and suprasellar tumor (5 x 4 x 3 cm) with mass effect but without invasive features or hydrocephalus (Figures 2, 3). The mass posteriorly displaced the upper brainstem, elevating the optic chiasm and cisternal portion of the bilateral optic nerves. The mass abutted and partially encased the cavernous, supra-clinoid portion of the bilateral internal carotid and basilar arteries and elevated the right P1 segment of the posterior cerebral artery without compromising vascular flow.
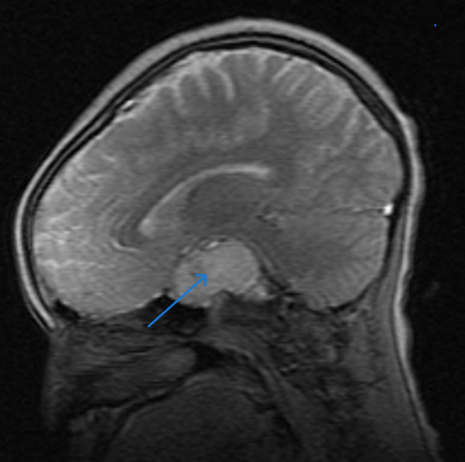
Figure 2. MRI of the sagittal section showing a suprasellar mass (arrow).
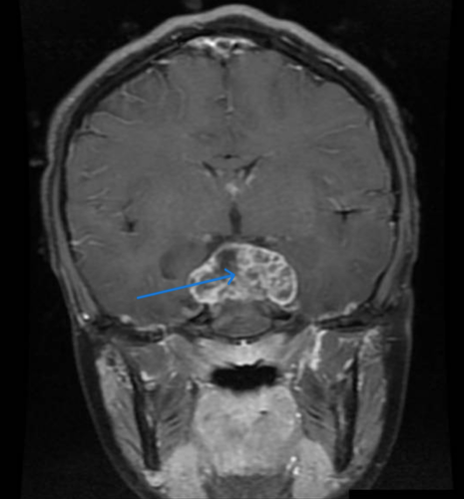
Figure 3. MRI of the coronal section shows a suprasellar mass (arrow).
While the initial CT and MRI were consistent with craniopharyngioma, histopathology from a transsphenoidal biopsy revealed features of chordoma: chords of neoplastic cells in a myxoid stroma and tumor cells with vacuolated cytoplasm. The positron-emission tomography (PET) CT ruled out tumor dissemination, and the neuro-ophthalmology assessment discovered myopia but no optic disc edema or pallor.
Differential Diagnosis.The differential diagnosis of suprasellar masses in children includes craniopharyngiomas, pituitary adenomas, germ cell tumors, and, rarely, malignant chordomas. All of these tumors can potentially cause visual changes and endocrine abnormalities. Craniopharyngiomas commonly include calcifications and cysts. Germ cell tumors are typically located more posteriorly, near the pineal gland, while pituitary adenomas reside within the sella turcica. Chordomas arise from the clivus, posterior and inferior to the sella turcica and pituitary gland.
Treatment and Management. After the tumor board discussion and family agreement, pediatric neurosurgery and otolaryngology performed a surgical resection of the clival chordoma via a nasal endoscopic transsphenoidal approach through the skull base. The patient’s surgical recovery was excellent, and she subsequently underwent radiation therapy, which she completed 2 months post-surgery.
Outcome and Follow-Up Post radiotherapy, the patient developed hypopituitarism, including central hypothyroidism, growth hormone deficiency, and delayed puberty. These complications are currently well-managed with thyroxine, growth hormone, and hormone replacement therapy. She was admitted 17 months after her initial surgery with cerebrospinal fluid (CSF) leaks, complicated by Haemophilus influenza meningitis. The leaks, likely due to radiation necrosis, were surgically repaired using fascia lata and fat grafting. Her bacterial meningitis was successfully treated with a 14-day course of ceftriaxone The patient is doing well 3 years post-resection with no neurological deficits. She receives a periodic brain MRI and shows no signs of recurrence.
Discussion. Chordomas are highly recurrent malignant tumors arising from notochordal remnants; they can develop in the cranial base, the sacrococcygeal region, and the vertebral column (Figure 4).1
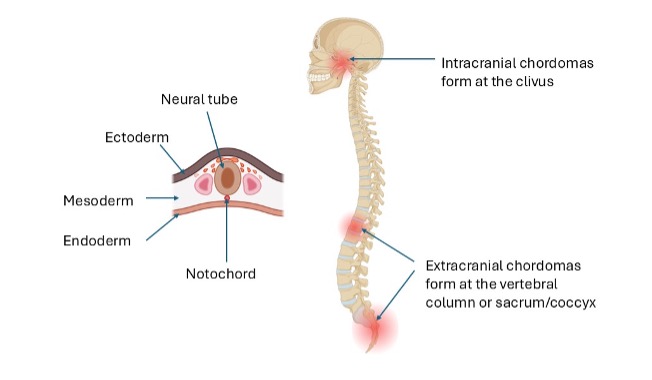
Figure 4. Chordomas are thought to arise from notochordal remnants (left). The image shows embryonic tissue origins, including neural tube, notochord, endoderm, mesoderm, and ectoderm. Chordomas develop intracranially, favoring the clivus, and extracranially at the vertebra or sacrum/coccyx (right).
Chordomas are rare in the general population (0.1% of all intracranial/skull-base tumors) and rarer in children, with less than 5% presenting in the first 2 decades of life.1,3,4-6, 19 When chordomas arise in children, the average age at diagnosis is 10 years.1 Chordomas appearing before age 5 are often aggressive, with a poor prognosis.1 Older children, however, often fare better than adults with chordomas.1,6-12 While adult chordomas favor sacrococcygeal locations, pediatric chordomas predominantly develop intracranially, on the sphenooccipital synchondrosis, first described by Lushka as “jelly-like” tumors at the clivus blumenbachii.1,2 Intracranial lesions have a better prognosis than vertebral lesions, which have a better prognosis than sacrococcygeal tumors.1 Sacro-coccygeal and spinal column tumors have a predilection for metastasis, spreading hematogenously or intrathecally through the subarachnoid spaces or ventricular shunting. Chordomas primarily metastasize to the lungs, then to bone, lymph nodes, skin, and liver.1
While early chordomas may be asymptomatic, intracranial chordomas arising from the clivus can cause visual disruption and headache from the mass effect on local structures. Sacrococcygeal chordomas can present with radiculopathy, bladder and bowel dysfunction, fulminant cauda equina syndrome, and an ulcerated subcutaneous mass.1 For cervical and thoracic lesions, an anterior tumor growth can present with respiratory dysfunction and/or dysphagia.1,13
Prior to surgery, a CT provides a critical assessment of bony involvement, while an MRI describes the proximity and involvement of critical soft-tissue structures.1,14 Surgical goals for a chordoma include a gross total resection and striving to remove any residual tumor from the adjacent neurovascular structures. Suprasellar masses arising from the clivus may be accessed via an endoscopic endonasal approach to the skull base, which can minimize complications. The clivus (Latin for “slope”) is a triangular-shaped bone formed from the basioccipital and basisphenoid bones at the spheno-occipital synchondrosis.15-18 The clival apex rests atop the cervical vertebrae, extending rostrally to separate the nasopharynx from the posterior cranial fossa. The superior clivus, formed by the dorsum sella and posterior clinoids, abuts the sella turcica, which houses the pituitary.16,18 The endoscopic extended endonasal approach allows faster and safer access to the clivus, with wider views compared to other microsurgical approaches.18
Following surgery, radiotherapy provides local control and increases survival rates in pediatric patients with a chordoma.23 Though toxicity rates are relatively low, radiation therapy to the skull base can result in pituitary abnormalities, particularly growth hormone deficiency and hypothyroidism.24 In addition, patients are at risk for injury to surrounding structures, including the brainstem, temporal lobe, and nearby blood vessels.24 Adjuvant radiation can also result in delayed radiation necrosis and subsequent CSF leaks requiring re-operation for repair.25 The combination of clival disruption for bony resection and radiation (necrosis) increases the risk of CSF leaks and intracranial infection.18, 20
Our patient presented for evaluation with a dry cough for 3 months, in the context of allergies and a recurrent upper respiratory tract infection. Was the cough truly a red herring prompting sinus imaging with a fortuitous incidental finding, or was it possibly a neurogenic cough from nerve root irritation? One report described a skull-based tumor presenting with cough and postnasal drip, with lesions discovered on CT imaging of the paranasal sinuses to evaluate acute sinusitis.22
The coughing reflex has afferent sensory nerve fibers, primarily vagal branches, that run directly to the medulla, upper brainstem, and pons. Efferent fibers exit the cough center via vagal, phrenic, and spinal motor nerves. The cough control center resides in the medulla, with orchestrating elements from the pontine respiratory group, the lateral tegmental field, and the deep cerebellar nuclei.21 Cerebral disorders associated with cough reflex hypersensitivity include dorsal medullary lesions (ie, Chiari I malformations), irritations of the cough center from mass effect, and autonomic dysregulation secondary to loss of parasympathetic innervation.21 An occult CSF leak from bony destruction of the clivus can cause a “post-nasal drip” related cough. While our patient did not have medullary extension, the mass effect had posteriorly displaced the upper brainstem.
The differential diagnosis of suprasellar masses in children typically includes craniopharyngiomas, pituitary adenomas, and germ cell tumors, with chordomas representing a rare but important class of skull-based tumors. This case illustrates how chordomas can mimic more common entities, such as craniopharyngiomas, both clinically and radiologically, as evidenced by the initial diagnostic impression. The suprasellar location and calcifications seen on imaging further complicated the preoperative assessment, underscoring the necessity of histopathological confirmation via biopsy.
In pediatric patients, where misdiagnosis can delay appropriate therapy and impact outcomes, maintaining a broad differential and pursuing a thorough workup are paramount. This experience reinforces the need for clinicians to consider less common skull-based tumors in children presenting with atypical or persistent symptoms, ensuring timely and tailored interventions. In this case, the child presented with an innocuous chronic cough, which, upon review of systems, was also associated with mild headache. Due to the astute history-taking and clinical work-up, we detected the tumor, and the child is now doing well, 3 years post-diagnosis.
Pediatric chordomas are rare, skull-based intracranial malignancies that pose surgical challenges due to their small size, their proximity to critical structures, the developing skull base, the lack of standardized guidelines, and limited case data. Treatment centers around maximal surgical excision. Endoscopic approaches minimize surgical complications to multiple critical adjacent structures. Adjuvant radiotherapy, standard for adult chordoma, is often used in pediatric cases, although its rarity makes standardization difficult. Ideal surgery clears residual tumor from neurovascular structures to minimize off-target effects of radiotherapy while permitting maximal dosing to prevent recurrence. Rare skull-based pediatric tumors should be described whenever possible to assist clinical decision-making, enhance available data, and improve patient outcomes. Mass effect from chordomas can cause unusual or innocuous presentations. Astute primary care clinicians are vital to the prompt detection of these conditions.
AUTHORS:
Nancy M. Gonzalez1 BA • Robert Mbilinyi1 MS • Lauren Culver,2 MD • Richard L. Byrd1,3MD
AFFILIATIONS:
1Texas A&M University Naresh K. Vashisht College of Medicine, College Station, TX, USA
2 Houston Methodist Hospital, Department of Neurosurgery, Houston, TX, USA
3 Kelsey-Seybold Clinic, Houston, TX, USA
CITATION:
Gonzalez NM, Mbilinyi R, Culver L, Byrd RL. Skull Base Tumor Presenting in a 10-Year-Old Girl with Cough. Consultant. Published online May 28, 2026. DOI: 10.25270/con.2026.05.000001
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Richard L. Byrd, Department of Pediatrics, Kelsey-Seybold Sienna Clinic, 7010 Hwy 6, Missouri City, TX 77459 (Richard.Byrd@kelsey-seybold.com)
References
- Beccaria K, Sainte-Rose C, Zerah M, Puget S. Paediatric chordomas. Orphanet J Rare Dis. 2015;10:116. doi:10.1186/s13023-015-0340-8
- Luschka P. Ueber gallertartige Auswüchse am Clivus Blumenbachii. Arch Pathol Anat Physiol Klin Med. 1857;11:8-12.
- Wold LE, Laws ER Jr. Cranial chordomas in children and young adults. J Neurosurg. 1983;59(6):1043-1047. doi:10.3171/jns.1983.59.6.1043
- Nix WL, Steuber CP, Hawkins EP, Stenback WA, Pokorny WJ, Fernbach DJ. Sacrococcygeal chordoma in a neonate with multiple anomalies. J Pediatr. 1978;93(6):995-998. doi:10.1016/s0022-3476(78)81235-9
- Sibley RK, Day DL, Dehner LP, Trueworthy RC. Metastasizing chordoma in early childhood: a pathological and immunohistochemical study with review of the literature. Pediatr Pathol. 1987;7(3):287-301. doi:10.1080/15513818709177131
- Borba LA, Al-Mefty O, Mrak RE, Suen J. Cranial chordomas in children and adolescents. J Neurosurg. 1996;84(4):584-591. doi:10.3171/jns.1996.84.4.0584
- O’Connell JX, Renard LG, Liebsch NJ, Efird JT, Munzenrider JE, Rosenberg AE. Base of skull chordoma: a correlative study of histologic and clinical features of 62 cases. Cancer. 1994;74(8):2261-2267. doi:10.1002/1097-0142(19941015)74:8<2261::aid-cncr2820740809>3.0.co;2-0
- Mitchell A, Scheithauer BW, Unni KK, Forsyth PJ, Wold LE, McGivney DJ. Chordoma and chondroid neoplasms of the spheno-occiput: an immunohistochemical study of 41 cases with prognostic and nosologic implications. Cancer. 1993;72(10):2943-2949. doi:10.1002/1097-0142(19931115)72:10<2943::aid-cncr2820721014>3.0.co;2-6
- Ridenour RV III, Ahrens WA, Folpe AL, Miller DV. Clinical and histopathologic features of chordomas in children and young adults. Pediatr Dev Pathol. 2010;13:9-17. doi:10.2350/09-01-0584.1
- Benk V, Liebsch NJ, Munzenrider JE, Efird J, McManus P, Suit H. Base of skull and cervical spine chordomas in children treated by high-dose irradiation. Int J Radiat Oncol Biol Phys. 1995;31:577-581. doi:10.1016/0360-3016(94)00395-2
- Hoch BL, Nielsen GP, Liebsch NJ, Rosenberg AE. Base of skull chordomas in children and adolescents: a clinicopathologic study of 73 cases. Am J Surg Pathol. 2006;30:811-818. doi:10.1097/01.pas.0000209828.39477.ab
- Grutza M, Lenga P, Issa M, et al. Pediatric skull base tumors: clinical features and surgical outcomes; a single-center retrospective study with a review of literature. Brain Spine. 2024;4:104136. doi:10.1016/j.bas.2024.104136
- Choi GH, Yang MS, Yoon DH, et al. Pediatric cervical chordoma: report of two cases and a review of the current literature. Childs Nerv Syst. 2010;26:835-840.
- Munari S, Colangeli R, Ramacciotti G, Zanoletti E. Clivus chordoma: case report and current considerations on treatment strategies. J Int Adv Otol. 2020;16(2):286-290. doi:10.5152/iao.2020.7494
- Rai R, Iwanaga J, Shokouhi G, et al. A comprehensive review of the clivus: anatomy, embryology, variants, pathology, and surgical approaches. Childs Nerv Syst. 2018;34(8):1451-1458. doi:10.1007/s00381-018-3875-x
- Rao D, Stein R, Jenson M, Patel J, Fiester P. Imaging review of the endoscopic operative corridor for clivus lesions. Curr Probl Diagn Radiol. 2023;52(1):66-76. doi:10.1067/j.cpradiol.2022.07.005
- Eisig SB, Goodrich JT. Cranial base surgery. Oral Maxillofac Surg Clin North Am. 2004;16(4):595-605. doi:10.1016/j.coms.2004.08.005
- Jozsa F, Das JM. Metastatic lesions of the clivus: a systematic review. World Neurosurg. 2022;158:190-204. doi:10.1016/j.wneu.2021.11.105
- Nayak JV, Thamboo A, Choby G, Harsh G, Hwang PH. Endoscopic management of clival chordomas and chondrosarcomas. In: Atlas of Endoscopic Sinus and Skull Base Surgery. 2nd ed. Elsevier; 2019:269-283. doi:10.1016/C2015-0-01193-5
- Warren Z, Roxbury C, Das P. Surgical management of spontaneous cerebrospinal fluid rhinorrhea arising from clival defects. In: Cerebrospinal Fluid Rhinorrhea. 1st ed. 2024:156-160.
- Al-Biltagi M, Bediwy AS, Saeed NK. Cough as a neurological sign: what a clinician should know. World J Crit Care Med. 2022;11(3):115-128. doi:10.5492/wjccm.v11.i3.115
- Douglas-Akinwande AC, Hattab EM. AJR teaching file: central skull base mass. AJR Am J Roentgenol. 2010;195(3 Suppl):S22-S24. doi:10.2214/AJR.07.7099
- Indelicato DJ, Rotondo RL, Mailhot Vega RB, et al. Local control after proton therapy for pediatric chordoma. Int J Radiat Oncol Biol Phys. 2021;109(5):1406-1413. doi:10.1016/j.ijrobp.2020.11.051
- Ioakeim-Ioannidou M, Niemierko A, Kim DW, et al. Surgery and proton radiation therapy for pediatric base of skull chordomas: long-term clinical outcomes for 204 patients. Neuro Oncol. 2023;25(9):1686-1697. doi:10.1093/neuonc/noad068
- Bresler AY, Mir G, Grube J, et al. Endoscopic paramedian forehead flap reconstruction of the anterior skull base for recalcitrant cerebrospinal fluid leaks: minimally invasive adaptation of ancient flap. World Neurosurg. 2019;130:37-41. doi:10.1016/j.wneu.2019.06.162
©2026 HMP Global. All Rights Reserved. Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Consultant360 or HMP Global, their employees, and affiliates.