
Peer Reviewed
Recurrent Retroperitoneal Liposarcoma: A Case Report on Surveillance Gaps and Recurrence
Introduction. A 62-year-old woman with a past medical history of a retroperitoneal liposarcoma presented to our free health clinic following a recent emergency department (ED) discharge for a left lower extremity deep venous thrombosis (DVT) and concerning imaging for a recurrent retroperitoneal liposarcoma.
History. At the free clinic, the patient endorsed left leg swelling and pain along with abdominal fullness, constipation, gas, nausea, and loss of appetite for the past month. In early 2022, the patient underwent surgical resection of a 27 cm primary retroperitoneal liposarcoma. Histopathological analysis revealed a mixed tumor composed of 60% well-differentiated and 40% dedifferentiated liposarcoma. The resection necessitated an en bloc left nephrectomy and total abdominal hysterectomy with bilateral salpingo-oophorectomy.
Postoperatively, the patient experienced a lapse in follow-up care due to the loss of insurance coverage. We did not obtain surveillance imaging until more than 1 year after her initial resection, when she sought care at a separate institution offering services to patients without insurance. In 2023, a contrast-enhanced CT of the abdomen and pelvis revealed 3 encapsulated, fat-containing, soft-tissue masses located within the retroperitoneum and pelvis: (1) 2.4 x 1.7 cm structure anterior to the left psoas muscle, (2) 3.3 x 1.8 cm structure along the posterolateral aspect of the left psoas muscle with soft tissue nodular densities, (3) 3.7 x 1.9 cm structure medial to the bifurcation of the left common iliac artery containing fat.
Shortly after we took the CT, the patient was displaced from her home and relocated to a different state to live with a family member. She also serves as the primary caregiver for her disabled son and is unable to work, further limiting her access to consistent medical care. Since relocating, the patient experienced another lapse in follow-up care due to the limited availability of healthcare resources for uninsured individuals in her new state of residence.
Approximately 1 month ago, the patient began experiencing new symptoms, prompting her decision to return to her original city of residence in hopes of re-establishing care at the local institution offering free health services. However, she was not eligible to receive medical care and must establish local residency for at least 3 months to qualify.
Eventually, the patient presented to the ED, where she was diagnosed with a left lower extremity DVT located in the external iliac vein. Additional work-up and imaging, including CT abdomen and pelvis with contrast, revealed a 19.4 x 10.1 x 13 cm pelvic lesion with a heterogeneous intrinsic appearance, most concerning for recurrence of the patient’s primary malignancy (Figure 1A-B).
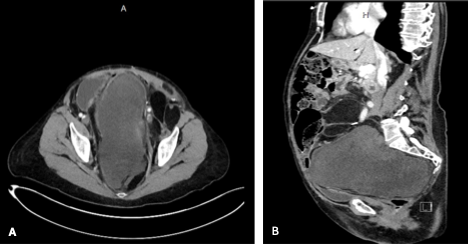
Figure 1. The CT of the abdomen and pelvis with contrast shows a heterogeneous pelvic lesion: (A) axial view, (B) sagittal view.
Additionally, imaging found mild hydronephrosis and hydroureter of the remaining right kidney (Figure 2A-B), likely secondary to compression by the pelvic mass. The lesion produced a mass effect on the adjacent bladder, which is otherwise grossly intact. Large fat globules were found throughout the retroperitoneum, displacing loops of bowel and causing right lateralization of the abdominal aorta. Finally, the lesion was causing a mass effect on the sigmoid colon, raising concern for a possible low-grade colonic obstruction contributing to the patient's reported constipation and bloating.
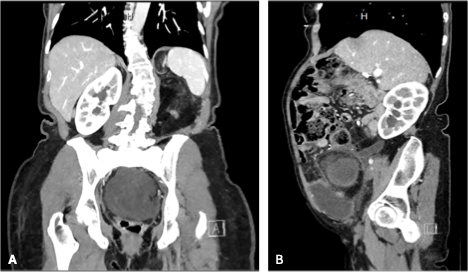
Figure 2. The CT of the abdomen and pelvis with contrast shows right hydronephrosis and hydroureter, (A) coronal view, (B) sagittal view.
Diagnostic testing: Following discharge from the ED, the patient presented to our free community health clinic (Figure 3). Upon presentation, the patient was hemodynamically stable: blood pressure 134/84 mmHg, heart rate 74 beats/min, temperature 36.6°C, height 157.5 cm, weight 60 kg, and oxygen saturation 95%. She is a well-appearing, age-appropriate woman in no acute distress. Her abdominal examination revealed significant distension, with preserved bowel sounds and no tenderness on palpation. All other physical examination findings were noncontributory. The patient’s laboratory tests were unremarkable, including white blood cell count, creatinine, BUN, aPTT, PT, and INR.
Based on CT imaging demonstrating a large, heterogeneous retroperitoneal mass, along with the patient’s abdominal distention and history of previously resected retroperitoneal liposarcoma, known for its high recurrence rate, the findings are highly suggestive of recurrent disease; however, definitive diagnosis requires histopathologic confirmation, which has not been obtained.
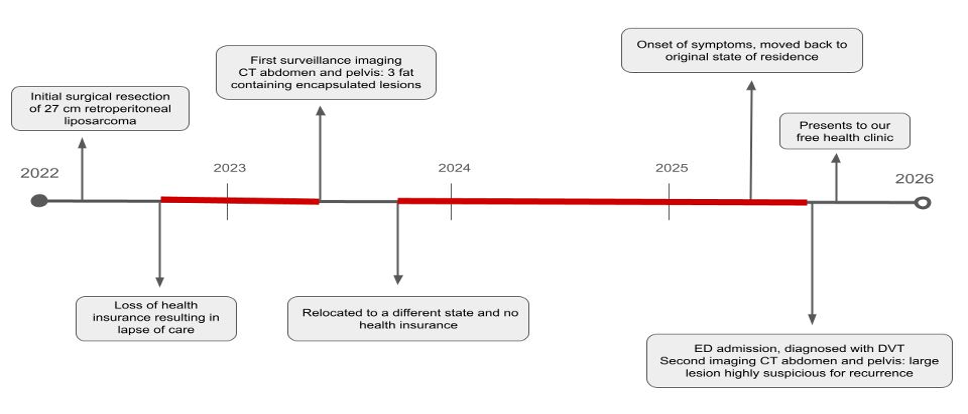
Figure 3. Pictured above is the patient's clinical timeline from 2022. The red markings indicate periods of lapse in surveillance imaging and follow-up care.
Differential diagnosis. Other potential considerations for the differential diagnosis of a retroperitoneal lesion include malignant tumors such as leiomyosarcoma, rhabdomyosarcoma, schwannoma, teratoma, and germ cell tumor, as well as benign fat-containing lesions such as angiomyolipoma or adrenal adenoma4,5. However, given the patient’s prior history of retroperitoneal liposarcoma, the presence of fat-containing components on CT imaging, and the known high risk of recurrence, particularly within the first few years post-resection, the current presentation is most consistent with recurrent retroperitoneal liposarcoma.
Treatment and management. Given her underlying hypercoagulable state, the patient was advised to continue apixaban therapy to reduce the risk of future thrombotic events. After a comprehensive clinical evaluation and review of available laboratory data, we recommended she pursue further management at a specialized tertiary care center capable of providing multidisciplinary sarcoma management and accommodating uninsured patients. The patient was provided with documentation and resources to facilitate the referral process and expedite access to care. Monthly follow-up visits were scheduled to monitor her condition, coordinate ongoing care, and reduce the risk of future loss to follow-up.
Discussion. Although soft tissue sarcomas (STSs) are rare malignant tumors, liposarcomas are the most common STS subtype globally and the predominant histopathological variant in the retroperitoneum, accounting for 41% of all retroperitoneal sarcomas.1,2 Retroperitoneal liposarcomas pose significant clinical challenges due to their deep anatomical location and slow but expansive growth. These tumors often remain asymptomatic until they have compromised or invaded adjacent organs. Despite complete surgical resection, the risk of local recurrence remains high and is the leading cause of death in retroperitoneal soft tissue sarcomas, in contrast to most other malignant tumors.3,4
Initial diagnostic evaluation typically involves imaging modalities, such as a CT and MRI. These tools help determine tissue composition, estimate tumor size, assess for metastatic spread, and evaluate involvement of vital structures. On CT, retroperitoneal liposarcomas generally appear as large, encapsulated masses with variable proportions of fat- and soft-tissue densities. An MRI is especially useful for evaluating vascular invasion, including the abdominal aorta and inferior vena cava, as well as lesions within the pelvis. Staging and distant metastasis can be monitored with chest CT scans, as the lungs are the most common site of metastasis. However, definitive diagnosis relies on histopathological examination and immunohistochemical analysis.3,5-7
Surgical resection with negative margins remains the cornerstone of treatment and frequently necessitates multiorgan resection, most commonly involving the kidney, as seen in the present case.7,8 Given the complex and infiltrative nature of these tumors, complete resection may be technically challenging. While the effectiveness of neoadjuvant or adjuvant radiotherapy and chemotherapy remains a topic of debate, these therapies may improve local control in selected cases.1,3,5,7 Current guidelines support close post-operative surveillance with physical examinations and total-body CT scans every 3-6 months for the first 2-3 years, as recurrence most often occurs within 6-48 months after initial treatment.1,2
Tumor histology is a prognostic factor in retroperitoneal liposarcomas. The most common subtypes are the well-differentiated (WDL) and dedifferentiated (DDL) subtypes, which account for over 90% of retroperitoneal liposarcomas and have 5-year survival rates of approximately 80% and 20%, respectively.3 Additionally, the heterogeneous composition of liposarcoma further complicates the therapeutic course, requiring individualized treatment plans. While researchers continue to investigate therapeutic strategies, there is currently no definitive guideline that offers optimal therapy for all presentations of retroperitoneal liposarcomas.4
Routine surveillance and comprehensive post-resection management are essential due to the high risk of recurrence and potential need for repeated surgical interventions. While current guidelines recommend surveillance imaging every 3–6 months following surgical resection of retroperitoneal liposarcoma, our present patient received only a single follow-up scan approximately 1 year postoperatively. She then remained without oncologic surveillance or management for the next 2 years due to loss of insurance and subsequent barriers to care. Her eventual re-presentation occurred during an emergency department visit for a newly diagnosed DVT, where imaging incidentally revealed a large recurrent retroperitoneal mass. The recurrent liposarcoma may have contributed to the patient’s hypercoagulable state, a common finding in malignancies due to various causes, including inflammation and tumor-specific prothrombotic mechanisms. Therefore, particular attention should be given to vulnerable populations, especially uninsured patients who are at increased risk for delayed diagnosis, loss to follow-up, and adverse outcomes. Enhanced post-treatment care protocols may include structured follow-up via regular outreach (eg, telephone reminders), increased access to adjuvant radiation and chemotherapy, and consideration of alternative screening strategies to detect early recurrence or secondary tumor development. Increased patient compliance can be achieved through individualized surveillance strategies that consider both clinical effectiveness and the patient’s perspective, such as cost and patient burden. Implementing frequent telephone follow-ups and physical examinations for patients unable to obtain CT imaging every 3–6 months can be an alternative screening strategy.9 Notably, these approaches are not substitutes for guideline-recommended imaging.
Additionally, early detection is crucial to reducing morbidity from complications, such as the DVT presented in our patient case, pulmonary embolism, stroke, renal failure, or spinal nerve impingement. As in the present patient case, many patients require en bloc resection of the ipsilateral kidney, which can lead to mild renal impairment, and should receive routine functional assessment of the remaining contralateral kidney. However, there is no standard protocol for monitoring kidney function post-resection.2,4,10 Given the complexity of retroperitoneal sarcomas, a multidisciplinary approach at specialized centers with integrated surgical, oncologic, radiologic, and supportive care services is recommended to optimize outcomes.
Conclusion. This case underscores the multifaceted challenges of managing recurrent retroperitoneal liposarcoma, particularly in uninsured patients with fragmented access to care. Despite aggressive initial resection, the patient experienced early recurrence, complicated by malignancy-associated venous thromboembolism and progressive mass effect. The absence of consistent surveillance and limited access to adjuvant therapies contributed to diagnostic delays and worsened prognosis. Effective management of retroperitoneal sarcomas requires not only multidisciplinary expertise and vigilant imaging follow-up, but also systemic strategies that address disparities in healthcare access. Ensuring affordable surveillance options, structured follow-up programs, and coordinated care pathways for vulnerable populations is essential to improving outcomes. Integrating a framework that includes low-cost imaging surveillance strategies, such as pelvic US screenings, and offering in-depth physical examinations at community-based health centers can help create more accessible follow-up care. This case highlights the critical intersection of clinical oncology, diagnostic imaging, and health equity in rare but aggressive malignancies.
AUTHORS:
Tooba Sheikh, BS1 • Zafar Qureshi, MD2 • Austine Leleji, BSc, MD3 • Syed A. Rizvi, MD, PhD, MPH, MBA3,4
AFFILIATIONS:
1FIU Herbert Wertheim College of Medicine, Miami, Florida, USA
2UMC Free Clinic, Miami Gardens, Florida, USA
3American International School of Medicine, Georgetown, Guyana, South America
4College of Biomedical Sciences, Larkin University, Miami, Florida, USA
CITATION:
Sheikh T, Qureshi Z, Leleji A, Rizvi AS. Recurrent retroperitoneal liposarcoma: a case report on surveillance gaps and recurrence. Consultant. Published online April 13, 2026. DOI: 10.25270/con.2026.04.000001
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE:
Syed A. A. Rizvi, MD, PhD, MPH, MBA. Larkin University. 18301 N Miami Ave, Miami, FL 33169 (srizvi@larkin.edu)
References
- Saha A, Habibullah Q, Rahman MM, et al. Retroperitoneal dedifferentiated liposarcoma – diagnostic and surgical challenges: a case report. Int J Surg Glob Health. 2025;8(2):e00546. doi:10.1097/GH9.0000000000000546
- Santangelo A, Fernicola A, Santangelo D, et al. Dark topics on giant retroperitoneal liposarcoma: a systematic review of 157 cases. Cancers (Basel). 2025;17(5):740. doi:10.3390/cancers17050740
- Mulita F, Verras GI, Liolis E, et al. Recurrent retroperitoneal liposarcoma: a case report and literature review. Clin Case Rep. 2021;9(9):e04717. doi:10.1002/ccr3.4717
- de Bree E, Michelakis D, Heretis I, et al. Retroperitoneal soft tissue sarcoma: emerging therapeutic strategies. Cancers (Basel). 2023;15(22):5469. doi:10.3390/cancers15225469
- Zafar R, Wheeler Y. Liposarcoma. In: StatPearls. StatPearls Publishing; 2025. Accessed September 26, 2025. NCBI Bookshelf. Zafar R, Wheeler Y. Liposarcoma. In: StatPearls. StatPearls Publishing; 2025. Accessed September 26, 2025. https://www.ncbi.nlm.nih.gov/books/NBK538265/
- Porrello G, Cannella R, Randazzo A, et al. CT and MR imaging of retroperitoneal sarcomas: a practical guide for the radiologist. Cancers (Basel). 2023;15(11):2985. doi:10.3390/cancers15112985
- Matthyssens LE, Creytens D, Ceelen WP. Retroperitoneal liposarcoma: current insights in diagnosis and treatment. Front Surg. 2015;2:4. doi:10.3389/fsurg.2015.00004
- Zhang WD, Liu DR, Que RS, et al. Management of retroperitoneal liposarcoma: a case report and review of the literature. Oncol Lett. 2015;10(1):405-409. doi:10.3892/ol.2015.3193
- Qiu M, Lin D, Xiong Z. Survival of a patient with five recurrences of retroperitoneal liposarcoma over a period of 13 years: a case report and review. Oncol Lett. 2023;26(2):367. doi:10.3892/ol.2023.1395
- Xue G, Wang Z, Liu B, et al. Short- and long-term post-nephrectomy outcomes for retroperitoneal liposarcoma from a high-volume sarcoma center: a propensity score matching analysis. Int J Clin Oncol. 2024;29. doi:10.1007/s10147-024-02530-2
©2026 HMP Global. All Rights Reserved. Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Consultant360 or HMP Global, their employees, and affiliates.