
Peer Reviewed
Iatrogenic Pneumocephalus, Intracranial Hypotension, and Cerebral Venous Sinus Thrombosis in a Postpartum Woman: A Unique Case
Introduction. A 22-year-old G1P1 woman with a BMI of 38 and no significant past medical history presented with severe frontal headache 2 days after an uncomplicated vaginal delivery with epidural anesthesia.
History. The patient described a throbbing frontal headache aggravated both by standing up and lying flat. Her headache was associated with photophobia, phonophobia, neck pain, and left upper extremity paresthesia with mild left arm and left leg weakness. The neurological examination was unremarkable, and her vital signs were within normal ranges except for a possible left arm drift.
Diagnostic Testing. The patient’s CT brain imaging revealed a small amount of air in both frontal horns of the lateral ventricles (Figure 1). Her brain CTA revealed distension of the superior sagittal sinus (SSS), inferior sagittal sinus, transverse sinus, and vein of Galen and an extra-axial SSS defect (Figures 2-4). The initial report of the MRI brain with and without contrast redemonstrated trace pneumocephalus but was otherwise unremarkable. Later review after 10 days, revealed pachymeningeal enhancement, venous sinus distension, and a filling defect in the SSS suggestive of venous sinus thrombosis (Figures 5, 6). Her MRI of the cervical spine did not reveal another cause of neck pain, and her urine protein was negative.
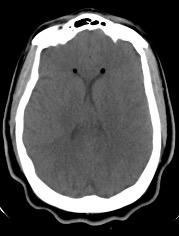
Fig. 1. Nondependent pneumoventricle within the bilateral frontal horns of the lateral ventricles.
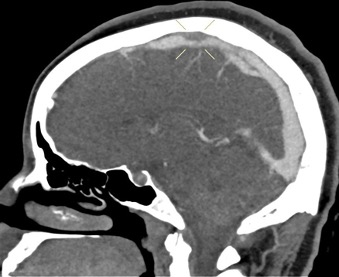
Fig. 2. Short segment filling defect of the mid portion of the superior sagittal sinus.
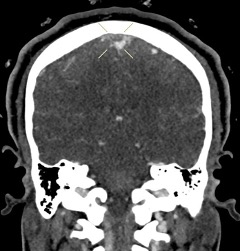
Fig. 3. Coronal view shows intraluminal filling defect of the superior sagittal sinus.

Fig. 4. Axial view of the focal filling defect compatible with thrombus within the superior sagittal sinus.
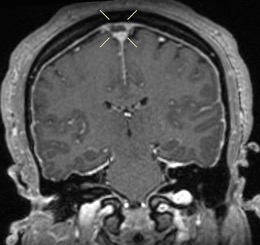
Fig. 5. Postcontrast coronal T1 images confirm the superior sagittal sinus filling defect seen on CT.
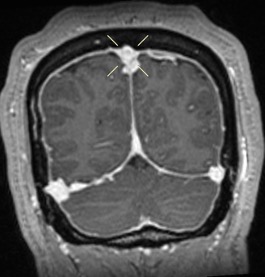
Fig. 6. Rounding and distention of the superior sagittal sinus and bilateral transverse sinuses.
After 10 days, the patient presented to the emergency department with continued severe headache, photophobia, blurry vision, and loss of balance. Her neurological examination revealed neck stiffness and left cheek numbness but was otherwise unremarkable. Her brain CTA identified interval development of complete SSS thrombosis (Figure 7). The second CTA, which revealed a thrombus in the SSS, confirmed the diagnosis of CVST.
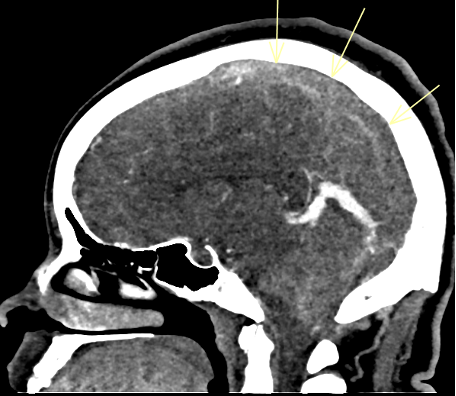
Fig. 7. Complete occlusive thrombosis of the superior sagittal sinus.
Differential diagnosis. The diagnosis of CVST may be overlooked because its only symptom may be headache, which affects approximately 35% of pregnant women and is usually benign2. However, severe etiologies of headache during pregnancy include CVST, pituitary apoplexy, post-lumbar puncture headache, pre-eclampsia, reversible cerebral vascular syndrome (RCVS), ruptured aneurysm, stroke, vertebral artery dissection, and others.
Post-lumbar puncture headache also occurs frequently and may follow epidural anesthesia. In this patient, the presence of pneumocephalus due to intradural puncture and MRI findings consistent with intracranial hypotension suggested post-lumbar puncture headache. Pre-eclampsia was considered, but the patient had normal blood pressure and no urine proteinuria.
Treatment and Management. Anticoagulant therapy with heparin was started, and the patient's headache improved. Follow-up imaging revealed development of bilateral subdural hygromas and persistent SSS thrombosis (Figure 8). Hypercoagulopathy work-up revealed borderline low Protein S, 41.1 [normal 63.5-149]. Hematology consultation suggested this abnormality was due to consumption in the acute setting and unlikely related to CVST. Protein C, cardiolipin Ab, beta-2 glycoprotein, and JAK2 were negative. The patient was discharged on oral anticoagulant therapy with rivaroxaban.

Fig. 8. Development of bilateral cerebral convexity subdural hygromas.
Outcome and follow-up. The plan was to continue anticoagulation and reassess clinically and with neuroimaging in 6 months. At her 6-month visit, she had no headache, a normal brain MRI, and no longer needed anticoagulation (Figures 9-11).
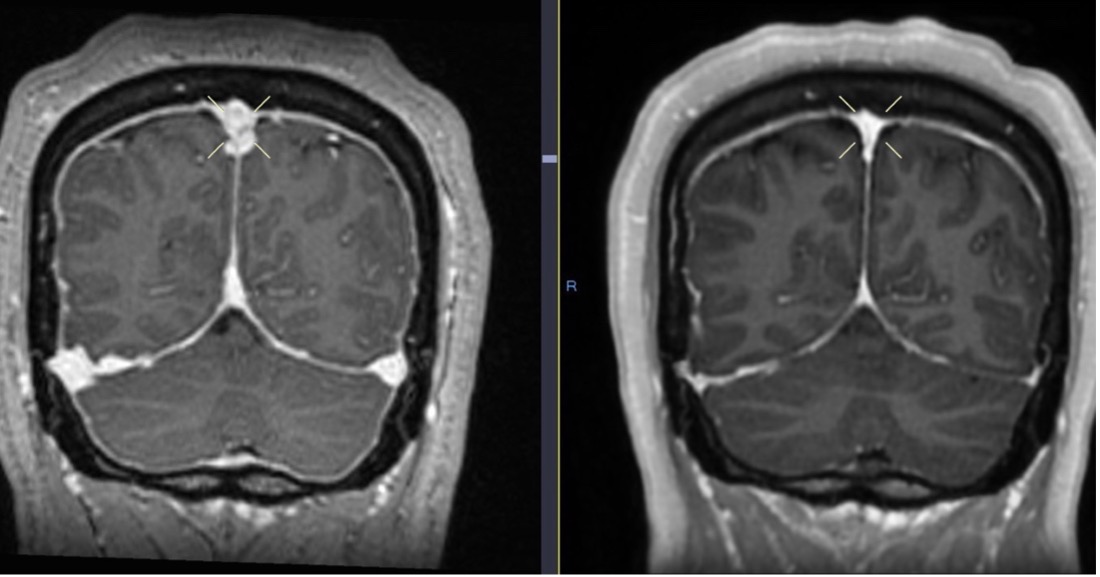
Fig. 9. Initial brain MRI (left) shows distention of the cerebral venous sinuses, with subsequent resolution 6 months later on follow-up MRI (right).
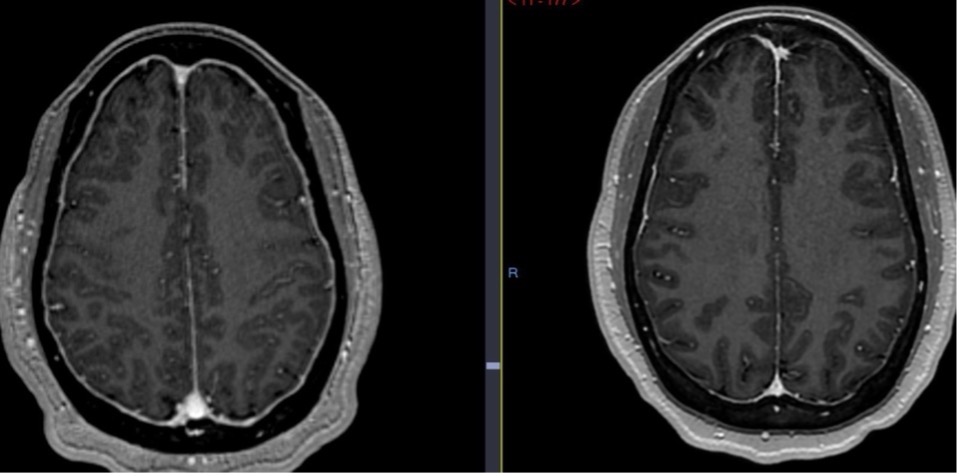
Fig. 10. Diffuse pachymeningeal thickening and enhancement on initial brain MRI (left), with interval resolution on follow-up MRI 6 months later (right).
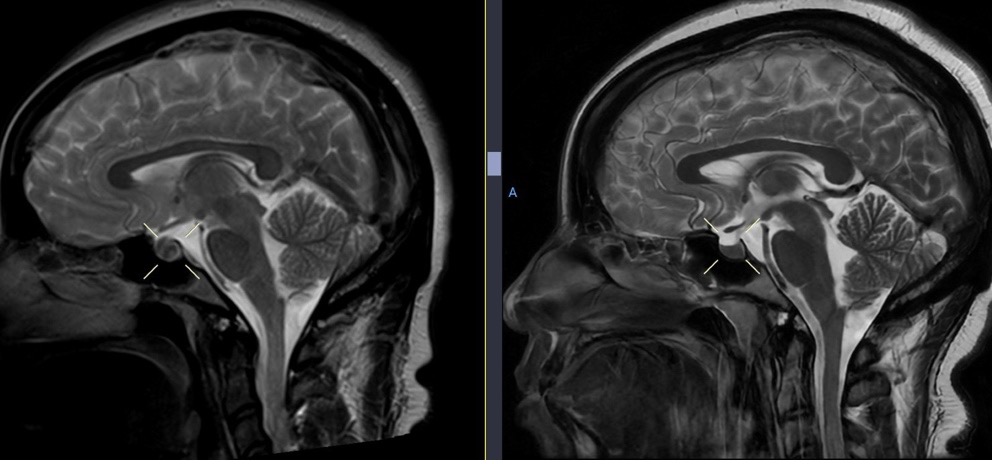
Fig. 11. Initial brain MRI (left) shows enlargement of the pituitary gland, with resolution on follow-up MRI 6 months later (right).
Discussion. Cerebral venous sinus thrombosis is a potentially life-threatening cause of stroke that accounts for approximately 1% of all strokes. It occurs with increased frequency in patients with coagulopathies, dehydration, intracranial tumors, systemic diseases, those taking oral contraceptives, during pregnancy, and the postpartum state1.
Pregnant and postpartum women are at increased risk of headaches and CVST. Headaches are also frequent after an intradural puncture. Pneumocephalus indicated this patient's epidural was intradural. Accidental dural puncture is an infrequent complication of epidural analgesia3. An inadvertent thecal hole or rent in epidural catheterization causes a cerebrospinal fluid (CSF) leak4. Pneumocephalus may result from dural puncture when air enters the CNS due to a ball-valve mechanism or inverted soda-bottle effect5.
This patient initially presented with headache, photophobia, neck pain, left upper extremity paresthesia, and later with blurred vision and loss of balance. These symptoms are suggestive of intracranial hypotension secondary to CSF volume loss4,6. Although not initially recognized, the brain MRI with and without contrast demonstrated classic signs of intracranial hypotension, including pachymeningeal enhancement, engorgement of dural venous sinuses, and pituitary enlargement4. These signs are subtle findings that may be easily overlooked if not searched for specifically. However, another classic feature of intracranial hypotension, bilateral subdural hematomas, developed later7. Brain sagging, which may be seen with intracranial hypotension, was not observed.
Intracranial hypotension is a risk factor for CVST8. Other risk factors include anemia, female gender, genetic thrombophilia, inflammatory disorders, malignancy, and obesity8. Our patient was female, postpartum, and obese. Her symptoms of headache, neck and low back pain, photophobia, and phonophobia are consistent with intracranial hypotension. Her headache was aggravated both by standing and lying flat, which is not typical for orthostatic headache or migraine. Her left upper extremity paresthesia and left arm and leg weakness were minimal and unexplained. These ultimately resolved and may have been secondary to CVST.
Pneumocephalus on CT post-epidural anesthesia should raise suspicion of an intradural puncture, CSF leak, and subsequent intracranial hypotension. Intracranial hypotension can provoke CVST in addition to other risk factors of the postpartum state. It is not known whether intracranial air can serve as a nidus for CVST development.
Conclusion. In summary, CSF leakage due to inadvertent dural puncture likely caused intracranial hypotension, which, in addition to the risk factors of the postpartum state and obesity, provoked SSS thrombosis9. This case illustrates that unexpected pneumocephalus in the setting of epidural anesthesia serves as a radiological marker of intradural puncture and CSF leak. Early recognition of CSF leak due to intradural puncture and treatment, such as with an epidural blood patch, might prevent intracranial hypotension and decrease the risk of CVST in this population10.
AUTHORS:
Linda Sherine Alfred, MD1 • Jenson Ma, MD2 • Khalid Khumage, MD 1 • Andrew Wilner, MD1
AFFILIATIONS:
1Neurology Department, University of Tennessee Health Science Center, Memphis, TN, USA
2Radiology Department, Regional One Health, Memphis, TN, USA
CITATION:
Alfred LS, Ma J, Khumage, K, Wilner A. Iatrogenic pneumocephalus, intracranial hypotension, and cerebral venous sinus thrombosis in a post-partum woman: A unique case. Consultant. Published online April 10, 2025. doi:10.25270/con.2025.05.000007
Received September 7, 2024. Accepted December 12, 2024.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE:
Linda Sherine Alfred, MD, 855 Monroe Avenue, Suite 415, Neurology Department, University of Tennessee Health Science Center, Memphis, TN, 38163 (lalfred1@uthsc.edu)
References
- Saadatnia M, Fatehi F, Basiri K, Mousavi SA, Mehr GK. Cerebral venous sinus thrombosis risk factors. Int J Stroke. 2009;4(2):111-23. doi:10.1111/j.1747-4949.2009.00260.x
- Raffaelli B, Neeb L, Israel-Willner H et al. Brain imaging in pregnant women with acute headache. J Neurol. 2018;265(8):1836-1843. doi:10.1007/s00415-018-8924-6
- Van de Velde M, Schepers R, Berends N, Vandermeersch E, De Buck F. Ten years of experience with accidental dural puncture and post-dural puncture headache in a tertiary obstetric anaesthesia department. Int J Obstet Anesth. 2008;17(4):329-35. doi:10.1016/j.ijoa.2007.04.009
- Mokri B. Spontaneous low pressure, low CSF volume headaches: spontaneous CSF leaks. Headache. 2013;53(7):1034-53. doi:10.1111/head.12149
- Thongtan T, Julayanont P, Test V. Pneumocephalus: a radiological presentation of intracranial hypotension secondary to spinal anaesthesia. BMJ Case Rep. 2021;14(1):e239750. doi:10.1136/bcr-2020-239750
- Chan SM, Chodakiewitz YG, Maya MM, Schievink WI, Moser FG. Intracranial hypotension and cerebrospinal fluid leak. Neuroimaging Clin N Am. 2019;29(2):213-226. doi:10.1016/j.nic.2019.01.002
- Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA. 2006;295(19):2286-96. doi:10.1001/jama.295.19.2286
- Edwards LS, Cuganesan R, Cappelen-Smith C. Cerebral venous thrombosis as a complication of intracranial hypotension after lumbar puncture. BMJ Neurol Open. 2020;2(2):e000046. doi:10.1136/bmjno-2020-000046
- Theofanis T, El-Chalouhi N, Tjoumakaris S. Cerebrospinal fluid leakage and cerebral venous sinus thrombosis: A case report. JHN Journ. 2013;8(1,2).
doi:10.29046/JHNJ.008.1.004 - van Kooten F, Oedit R, Bakker SL, Dippel DW. Epidural blood patch in post dural puncture headache: a randomised, observer-blind, controlled clinical trial. J Neurol Neurosurg Psychiatry. 2008;79(5):553-8. doi:10.1136/jnnp.2007.122879