
Peer Reviewed
An Abnormal Constellation of Electrocardiographic and Metabolic Manifestations in an Unusual Presentation of Encephalopathy
Introduction. A 32-year-old woman with a past medical history of anemia and a significant trauma history presented to the hospital in March 2025 with subacute progressive isolation, anorexia, audiovisual hallucinations, and religious preoccupation, after being found unresponsive in her apartment with urinary incontinence.
History. According to external reports from family, friends, and neighbors, the patient began having a subacute change in her personality in January 2025, which resulted in her becoming more withdrawn and exhibiting behaviors indicative of increasing social isolation (e.g. ceasing all contact with family and friends).
Approximately 3 months after the onset of her symptoms, the patient began to refuse to eat and started experiencing audiovisual hallucination. Her condition continued to rapidly deteriorate until she was found by her building manager unconscious on the floor, soaked in urine, with further development of nonbloody and nonbilious vomiting en route to the hospital by emergency medical services.
On the physical examination completed during initial admission, the patient had findings notable for significant psychomotor slowing with bradykinetic movement, flat affect, stupor, vertical and lateral nystagmus. Additionally, her neurological examination was significant for brisk patellar reflexes (R > L) without clonus, and slight resistance to passive range of movement. There was no evidence of peripheral neuropathy given that she had more than two reflexes with sensations grossly intact. The patient’s physical examination was also notable for mild memory changes given the fact that she endorsed and showed delays in thought processing and memory recall. The patient’s urine toxicology and drug screening were unremarkable and unrevealing. The patient’s history of weight loss due to decreased intake could not be obtained because of the patient’s mental status on admission.
Diagnostic testing. Given the patient’s clinical condition, the patient had diagnostic laboratory testing and imaging completed on admission. The patient’s tests were significant for lactic acidosis, hypokalemia, hypophosphatemia, hypomagnesemia, and elevated levels of beta-hydroxybutyrate (normal range, < 0.4 - 0.5 mmol/L).
The patient’s imaging diagnostics were significant for a head CT that showed high-density foci in the globi pallidi, right greater than left, likely reflecting calcification (Figure 1) and a brain MRI completed on initial admission in late March that was significant for grossly abnormal subcortical enhancement with associated T2/Flair hyperintensity noted in the bilateral medial thalami, posterior putamen, midbrain, substantia nigra, and periaqueductal gray matter (Figure 2). On initial admission, clinicians performed an EKG, which was significant for diffuse T-wave inversions in the inferior and precordial leads (e.g. cerebral T-waves) that resolved on repeat testing (Figure 3).
Given the following diagnostics, despite the unusual clinical presentation, the most likely underlying etiology of the patient’s clinical manifestations is Wernicke encephalopathy (WE).

Figure 1. CT Head completed on day of initial admission. Findings significant for high density foci in the right global palladi that likely reflects calcification/mineralization
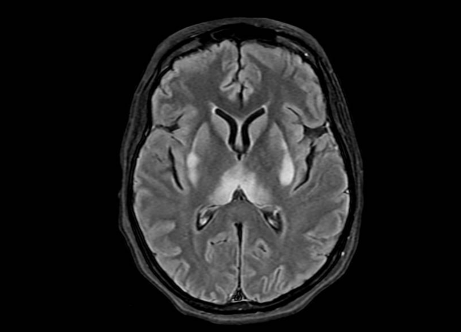
Figure 2. MRI Brain (with and w/o contrast) on day of initial admission before treatment. MRI Brain showing symmetric restricted diffusion with associated T2/FLAIR hyperintensity noted in bilateral medial thalami, posterior putamen, midbrain (including the substantia nigra) and periaqueductal gray. Additional subtle T2/FLAIR hyperintensity without corresponding restricted diffusion noted dorsal medulla. No associated enhancement.
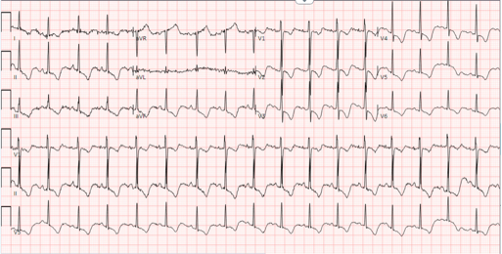
Figure 3. Abnormal findings seen on electrocardiogram (ECG) completed on initial admission to the hospital. ECG significant for deep T-wave inversions on the inferior leads (II, III, avF) and the precordial leads (V1-V6). These cerebral T-waves lend credence to brain parenchymal injury and point the diagnosis more towards Wernicke’s encephalopathy.
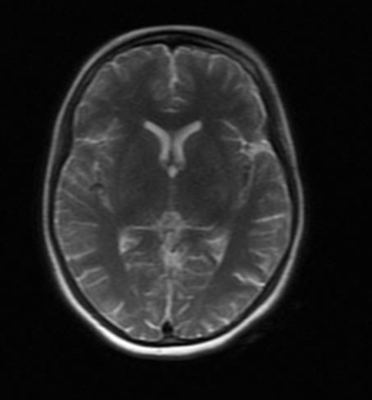
Figure 4. MRI Brain approximately 1 week after treatment with 400 mg IV thiamine TID. MRI Brain (with and without contrast) shows significantly improved restricted diffusion at the bilateral putamen, medial thalami, and substantia nigra. Abnormal enhancements are significantly reduced.
Differential diagnoses. Given the fact that the patient was found unresponsive in her apartment with urinary incontinence and was found to have hypokalemia, lactic acidosis, abnormal head CT/brain MRI, and cerebral T-waves on EKG during initial admission, there was concern for a possible provoked seizure. The etiology of the possible provoked seizure was unclear on initial admission, and the differential diagnosis was broad. The possible provoked seizure was thought to be from a sequela of nutritional derangements secondary to an underlying neuropsychiatric disorder, such as depression or psychosis, with the patient’s bradykinetic movement and concurrent psychomotor slowing thought to be a consequence of WE secondary to and worsened by severe malnutrition in the setting of decreased intake.
The patient’s WE diagnosis was primary on our list (both as a primary condition and underlying condition) given the patient’s abnormal physical examination findings of dysconjugate gaze, vertical gaze nystagmus, altered mental status, and her abnormal brain MRI findings significant for T2/FLAIR hyperintensities of the medial thalami and periaqueductal gray matter.
Other differential diagnoses that were taken into consideration attempted to unify the patient’s neurological and psychiatric symptoms such as Creutzfeldt-Jakob disease (CJD), which is a a fatal and rapid neurodegenerative disease process notable for akinetic mutism, hallucinations, seizures with imaging findings significant for thalamic and basal ganglia enhancement on T2/FLAIR MRI (with restricted diffusion enhancement). The patient’s similar symptoms, alongside her personality changes and her urinary incontinence, was somewhat concerning for this disease process. However, the lack of myoclonus, muscle spasms and twitches, and the patient’s rapid improvement after treatment made this diagnosis far less likely.
Autoimmune (anti-NMDAR) encephalitis, viral encephalitis, and Wilson disease were also part of the differential diagnosis but given the patient’s duration of symptoms, negative biomarkers, lack of meningeal fevers, and rapid improvement after being treated these diagnoses proved to fall lower in order of priority on the differential diagnosis.
Treatment and management. Given the primary and significant concern for Wernicke encephalopathy (alongside her nutritional derangements), the patient was initiated on high-intensity intravenous (IV) thiamine repletion (400 mg IV three times a day) and had her electrolytes aggressively replenished given her electrolyte and nutritional derangements on initial admission. Additionally, a serum ceruloplasmin, rapid plasma reagin, HIV, antinuclear antibody, and a serum and cerebrospinal autoimmune panel were ordered for further study to rule out other diagnoses given the patient’s broad differential and unclear etiology initially on presentation.
After approximately 1 week of IV thiamine repletion, the patient’s overall clinical condition improved significantly, and a brain MRI (T2-weighted) completed 1 week later showed significant improvement from the previous findings (Figure 4). Considering the patient’s psychiatric symptoms on initial admission and the concern for an underlying depression or psychosis, the patient was initiated on escitalopram 10 mg daily and, briefly, quetiapine, which was discontinued after 2 days following a significant overall improvement in the patient’s Wernicke encephalopathy and metabolics.
Outcome and follow-up. After intensive thiamine initiation, aggressive electrolyte repletion, and a trial of antidepressants, the patient’s overall condition greatly improved, and she returned to her baseline condition. The patient was discharged in late April 2025 after prolonged disposition related to experiencing homelessness. At discharge, she was continued on oral thiamine of 100 mg and oral escitalopram 10 mg. She was scheduled for a follow-up appointment with outpatient psychiatry. Despite the scheduled appointment, the patient was lost to follow-up but, fortunately, has not returned to the hospital with additional medical issues.
Discussion. This case illustrates a striking and atypical presentation of WE in a 32-year-old woman with significant trauma history, but no history of alcohol use—a key risk factor typically associated with WE. Her subacute psychiatric and neurologic decline, culminating in stupor, urinary incontinence, nystagmus, and imaging abnormalities, highlights both the protean nature of this condition and the critical importance of timely recognition and intervention.
Essential features of the presentation included a months-long evolution of personality change, progressive social withdrawal, anorexia, and hallucinations—symptoms initially suggestive of a primary psychiatric disorder. However, the discovery of metabolic derangements (lactic acidosis, hypokalemia, hypomagnesemia, hypophosphatemia), signs of central nervous system involvement (vertical nystagmus, bradykinesia, stupor), EKG abnormalities, and pathognomonic MRI findings—particularly T2/FLAIR hyperintensities in the bilateral medial thalami, midbrain, and periaqueductal gray matter—ultimately pointed toward a metabolic encephalopathy, with WE as the underlying diagnosis despite the fact that this patient’s presentation did not perfectly align with the classical clinical triad found in WE: altered mental status, oculomotor abnormalities, and ataxia.1
In the literature, WE remains underdiagnosed in in individuals without alcohol use disorder. While classically described in patients with chronic alcohol use disorder, mounting evidence supports that malnutrition from psychiatric illness, gastrointestinal disease, and bariatric surgery (e.g. gastric bypass) are increasingly recognized contributors.1,2,3 Indeed, WE among in individuals without alcohol use disorder often involves a delayed diagnosis due to its subtler or more variable presentation, especially when psychiatric symptoms obscure the clinical picture.4,5 Similar to findings from Zuccoli et al.6, this case reinforces that MRI—particularly diffusion-weighted and FLAIR imaging—is an invaluable diagnostic adjunct, capable of identifying characteristic lesions even in the absence of the classic clinical triad (ophthalmoplegia, ataxia, confusion), which is seen in only ~10% of patients.7,8 The reversibility of both clinical, radiologic, and electrocardiographic abnormalities with prompt thiamine repletion is also well documented and echoed within this case.9,10
Conclusion. The rationale for reporting this case lies in its multidimensional educational value. First, it provides a compelling demonstration of WE among an individual without alcohol use disorder presenting primarily with psychiatric symptoms, challenging the cognitive bias toward psychiatric diagnoses in young women with trauma histories. Second, it underscores the risk of refeeding syndrome and the necessity of electrolyte monitoring and correction in nutritionally compromised patients. Third, it calls attention to the diagnostic power of neuroimaging and electrocardiographic analysis (e.g. cerebral T-waves) and the importance of high clinical suspicion in the face of ambiguous presentations. Finally, the case serves as a potent reminder that WE is a medical emergency, and delays in treatment can result in irreversible neurological damage, including Korsakoff syndrome.
This case also highlights key lessons. For example, clinicians should assess the nutritional status of patients with psychiatric disorders, especially with signs of food refusal or neglect. It underscores the need for a biopsychosocial approach, as neurological disorders can mimic psychiatric illness. The variable, reversible nature of WE challenges diagnostic assumptions and urges physicians to stay flexible, considering treatable medical causes behind psychiatric symptoms.
AUTHORS:
Chisom Enwere, MD1 • Julie Wong2
AFFILIATIONS:
1Columbia University Vagelos College of Physicians and Surgeons; Icahn School of Medicine at Mount Sinai
2Columbia University Undergraduate Student
CITATION:
Enwere C, Wong J. An abnormal constellation of electrocardiographic and metabolic manifestations in an unusual presentation of encephalopathy. Consultant. Published online September 15, 2025. doi:10.25270/con.2025.09.000001
Received May 8, 2025. Accepted June 26, 2025.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE:
Chisom Enwere MD, Columbia University Vagelos College of Physicians and Surgeons, 788 Columbus Avenue, NY, NY 10025 (chisom.enwere@gmail.com)
References
- Sinha S, Kataria A, Kolla BP, Thusius N, Loukianova LL. Wernicke encephalopathy—clinical pearls. Mayo Clin Proc. 2019;94(6):1065-1072. doi:10.1016/j.mayocp.2019.02.018
- Manzo G, De Gennaro A, Cozzolino A, Serino A, Fenza G, Manto A. MR imaging findings in alcoholic and nonalcoholic acute Wernicke encephalopathy: a review. Biomed Res Int. 2014;2014:503596. doi:10.1155/2014/503596
- Oudman E, Wijnia JW, Oey MJ, van Dam M, Postma A. Wernicke-Korsakoff syndrome despite no alcohol abuse: a summary of systematic reports. J Neurol Sci. 2021;426:117482. doi:10.1016/j.jns.2021.117482
- Scalzo SJ, Bowden SC, Ambrose ML, Whelan G, Cook MJ. Wernicke-Korsakoff syndrome not related to alcohol use: a systematic review. J Neurol Neurosurg Psychiatry. 2015;86(12):1362-1368. doi:10.1136/jnnp-2014-309598
- Kohnke S, Meek CL. Don’t seek, don’t find: the diagnostic challenge of Wernicke encephalopathy. Ann Clin Biochem. 2021;58(1):38-46. doi:10.1177/0004563220939604
- Zuccoli G, Pipitone N. Neuroimaging findings in acute Wernicke encephalopathy: review of the literature. AJR Am J Roentgenol. 2009;192(2):501-508. doi:10.2214/AJR.07.3959
- Liu YL, Xiao WM, Liang MQ, Wu ZQ, Wang YZ, Qu JF, Chen YK. Clinical characteristics and magnetic resonance imaging findings in nine patients with nonalcoholic Wernicke encephalopathy: a retrospective study. Neuropsychiatr Dis Treat. 2019;15:2433-2441. doi:10.2147/NDT.S217237
- Wijnia JW. A clinician’s view of Wernicke-Korsakoff syndrome. J Clin Med. 2022;11(22):6755. doi:10.3390/jcm11226755
- Cornea A, Lata I, Simu M, Rosca EC. Wernicke encephalopathy presenting with dysphagia: a case report and systematic literature review. Nutrients. 2022;14(24):5294. doi:10.3390/nu14245294
- Alves Pereira de Carvalho Saraiva R, Gonçalves M, Sereijo C, Mendes T, Kamyar RB, Abreu M, Coentre R. Nonalcoholic Wernicke-Korsakoff syndrome resulting from psychosis. J Nerv Ment Dis. 2021;209(3):229-231. doi:10.1097/NMD.0000000000001287