
Peer Reviewed
Identification of a Chronic Lower Extremity Wound in a Patient With a Mechanical Valve
Introduction: A 54-year-old woman with a history of mitral valve replacement and warfarin therapy presented to the emergency department with worsening right lower extremity pain.
History. One year prior to this current admission for worsening right lower extremity pain, the patient was hospitalized for right knee septic arthritis, which was complicated by methicillin-sensitive Staphylococcus aureus (MSSA) bacteremia and endocarditis. The patient underwent a mitral valve replacement for severe mitral valve regurgitation with a large vegetation secondary to endocarditis. She was initiated on 5 mg daily warfarin anticoagulation therapy and, within a month, developed ulcers of her right lower extremity. She remained on warfarin because of the need for ongoing anticoagulation for her mechanical mitral valve.
Three months prior to this current admission for worsening pain, she was hospitalized for the second time for recurrent MSSA bacteremia related to her chronic leg wound. At the time of her second admission, a biopsy of her ulcer was performed (Figure 1), which was reviewed at the time of her current admission (Figure 2).
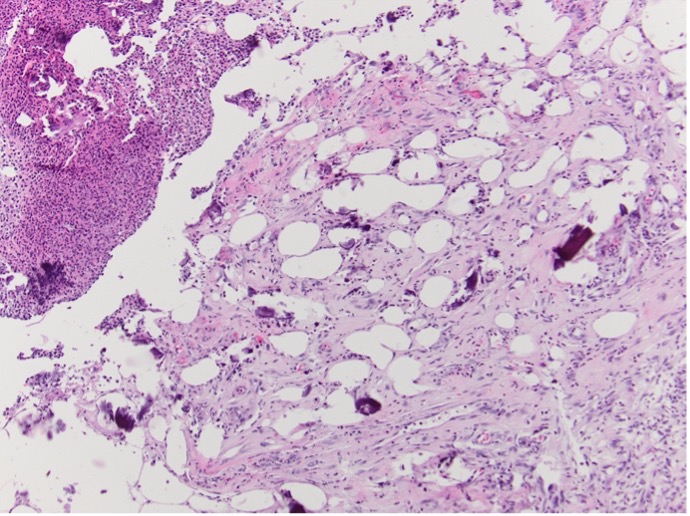
Figure 1. Ulceration extends into the panniculus. Calcification is noted (Hematoxylin-eosin-stained sections; original magnification x100).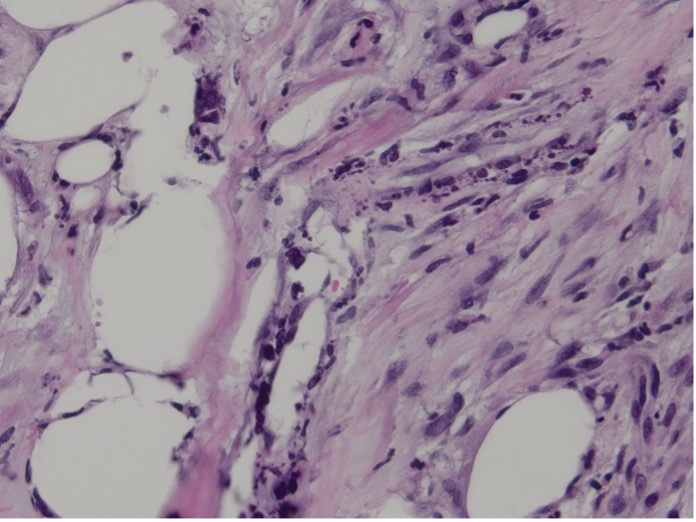
Figure 2. Calcification is noted in the walls of small blood vessels (Hematoxylin-eosin-stained sections; original magnification x400).She presented with worsening pain but was afebrile and hemodynamically stable (temperature 36.6 °C, heart rate 91 bpm, blood pressure 91/68 mm Hg, SpO₂ 97%). Her examination revealed multiple large erosions on the right calf without purulence or necrosis (Figure 3). Review of medications showed she was still anticoagulated on warfarin.

Figure 3. An image of the patient’s right lower extremity wounds at the time of admission.Diagnostic Testing. Laboratory studies revealed a non–anion gap metabolic acidosis (bicarbonate 14 mmol/L, pH 7.22) with mild leukocytosis (12 ×10³/µL) and elevated creatinine (1.9 mg/dL; baseline 1.2 mg/dL). Calcium was within normal range (10 mg/dL), and her phosphate level was elevated. Blood cultures were negative. CT of the right lower extremity showed cellulitis overlying chronic ulcerations without abscess or thrombosis. She was started on cefepime and vancomycin for Pseudomonas and methicillin-resistant Staphylococcus aureus coverage. During this time, she also remained on warfarin.