
Peer Reviewed
Facial Swelling and Linear Vesicles in a Pediatric Patient
Introduction. A 9-year-old boy presented to the emergency department (ED) with a facial eruption that emerged following a weekend camping trip.
History. Four days after the trip, the patient developed a progressively worsening rash that initially involved the face characterized by erythema, edema, and pruritus. The patient also developed lesions on the trunk and proximal extremities.
Given the significant facial edema and erythema, there was concern for an infectious process including periorbital or orbital cellulitis. The patient did not have painful extraocular movements, so a diagnosis of periorbital cellulitis was favored, and he was discharged home with a 5-day course of oral trimethoprim-sulfamethoxazole and hydrocortisone 2.5% cream administered daily on the lesions. The patient had a documented allergy to cephalexin.
Two days later, the patient re-presented to the ED due to worsening symptoms and the development of new lesions on the trunk despite proper adherence to the prescribed medications. On examination, the patient had increased facial and periorbital edema, erythema, and yellow to light brown serum exudate (Figure 1). A thorough physical examination revealed additional edematous, linear, scaly plaques on the patient's neck, chest, abdomen, shoulder, penis, and left thigh (Figure 2).

Figure 1. Pink, erythematous and edematous plaques with yellow to light brown exudate and crusts involving the forehead, bilateral cheeks and left periorbital skin.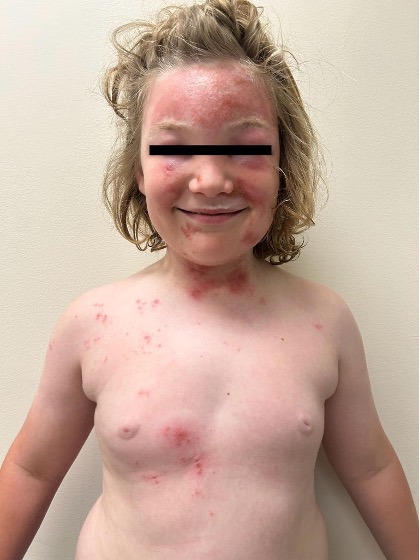
Figure 2. A well appearing patient with pink papules and vesicles with excoriations coalescing into linear plaques on the face, trunk and proximal extremitiesGiven these findings, the patient was prescribed a new regimen of antibiotics with oral amoxicillin-clavulanic acid and topical mupirocin. Dermatology was consulted for further evaluation.
Diagnostic testing. Bacterial cultures were obtained to evaluate for impetiginization of the dermatitis, and a herpes simplex virus (HSV) lesional swab for polymerase chain reaction (PCR) was obtained. These evaluations were both negative.