
Early, Higher Methadone Dosing May Reduce Risk of Patient-Directed Discharge in Hospitalized Patients With OUD
Key Highlights:
- Higher methadone dosing within the first 72 hours significantly reduced early patient directed discharge (PDD).
- Elevated opioid withdrawal scores were strongly associated with higher rates of early PDD.
- Buprenorphine showed a protective effect only at the 72-hour mark, not earlier.
- Nearly 7% of opioid use disorder (OUD)-related hospitalizations ended in PDD within 72 hours.
A retrospective observational study presented at the Society of Hospital Medicine Converge in Las Vegas, NV, identified a strong association between early dosing of medications for opioid use disorder (MOUD)—particularly methadone—and the risk of PDD within 72 hours of hospital admission. Patients who received higher methadone doses in the initial days of hospitalization had significantly reduced odds of early PDD. Similarly, a higher 72-hour buprenorphine dose was linked to better retention.
According to the study authors, up to 25% of hospitalizations among individuals with OUD result in early self-discharge. Although previous studies have found that MOUD reduces PDD risk, evidence on how dosing and timing affect this outcome have been limited. This study aimed to address that gap and optimize care continuity.
For their study, researchers reviewed hospital records from Johns Hopkins Hospital between July 2019 and June 2022. Adults with an OUD-related ICD-10 diagnosis and oral/sublingual MOUD use were included, excluding those who left after 72 hours. Demographic data, Clinical Opiate Withdrawal Scale (COWS) scores, and medication details were extracted from the electronic medical record. The main outcome was PDD within 72 hours.
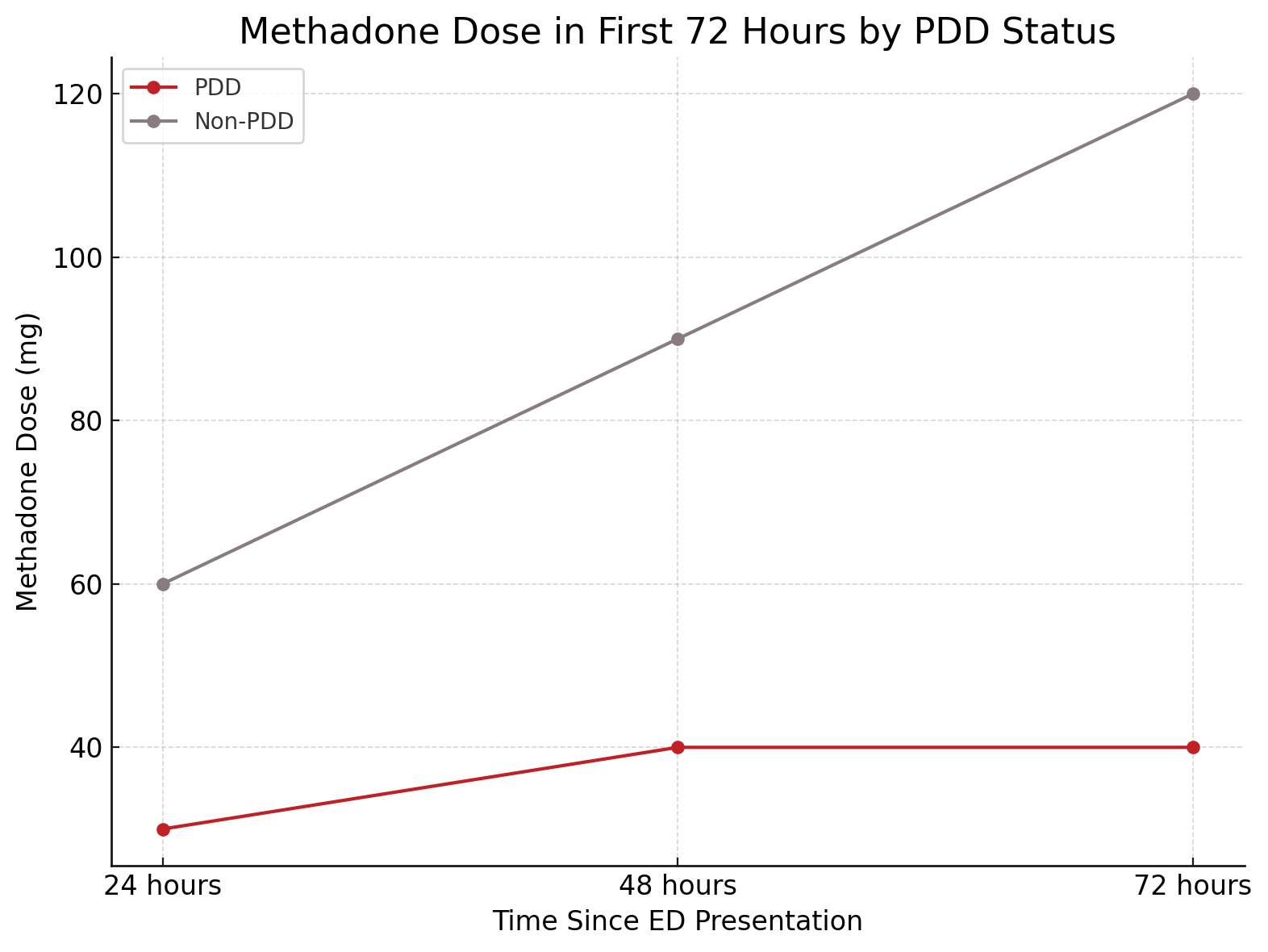
Out of 4134 encounters, 6.8% ended in early PDD. Patients who left early had significantly higher median COWS scores (12 vs 2, P < .001), indicating more severe withdrawal. Methadone dosing was notably lower in the PDD group at every 24-hour increment up to 72 hours (30 mg vs 60 mg at 24 hours; 40 mg vs 120 mg at 72 hours). Buprenorphine differences were only significant at 72 hours (11.7 mg vs 20 mg, P = .006).
“Our study findings support the hypothesis that undertreated opioid withdrawal (higher COWS) is associated with higher risk of PDD,” the researchers concluded. “More work is needed to understand safe and effective inpatient dosing strategies for MOUD, as well as the role of adjunctive medications and short-acting opioids.”
Reference:
Meredith R, Garneau WM, Buresh M. Association of first 72-hour MOUD dose and timing with patient directed discharge. Presented at: Society of Hospital Medicine Converge; 2025; Las Vegas, NV. Accessed April 22, 2025. https://shmabstracts.org/abstract/association-of-first-72-hour-moud-dose-and-timing-with-patient-directed-discharge/.