
Comparing CBO, DTC Delivery of the Keep It Up! Digital HIV Prevention Program
Key Highlights
- In a pragmatic trial of 2,124 YMSM, DTC enrolled more participants overall, while CBO delivery reached higher proportions of Black and Latino participants.
- Adherent PrEP (aPrEP) use rose in both arms by 12 weeks, with a larger increase in the CBO arm.
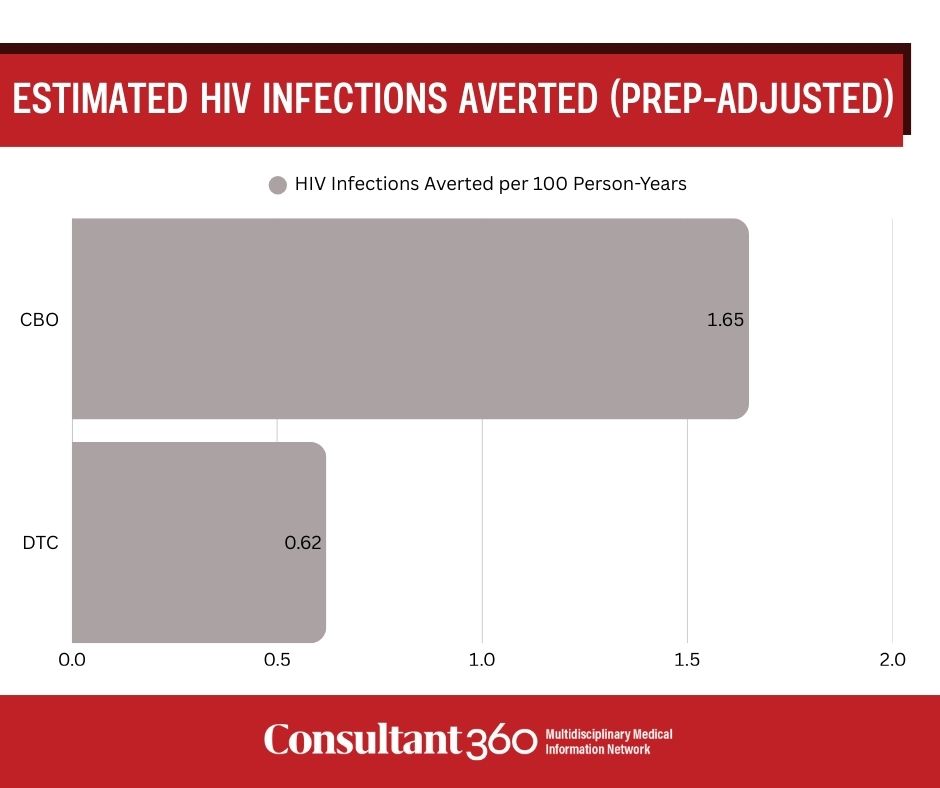
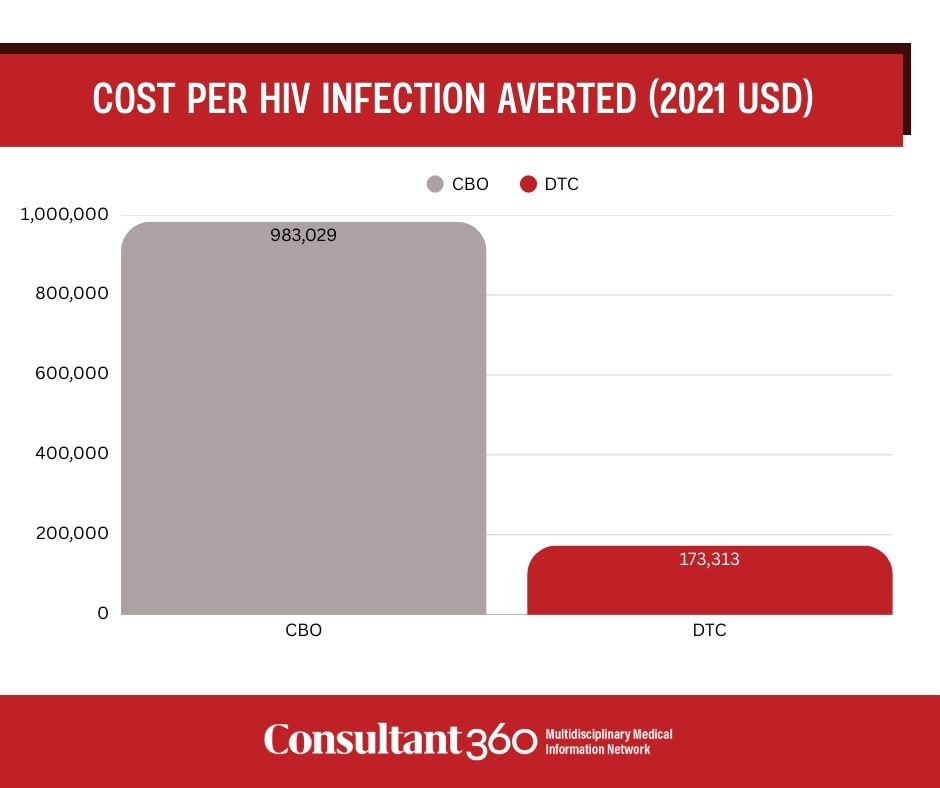
- Estimated HIV infections averted (PrEP-adjusted) were higher in the CBO arm than DTC, but cost per infection averted was substantially higher for CBO than DTC.
A large type III hybrid effectiveness–implementation trial published in AIDS and Behavior compared two real-world strategies for delivering Keep It Up! (KIU!), a CDC-classified digital HIV prevention intervention for young men who have sex with men (YMSM). The trial randomized 66 U.S. counties and enrolled 2,124 participants between December 2019 and March 2023 to evaluate implementation reach, short-term effectiveness, and costs per HIV infection averted.
Participants aged 18–34 years who were HIV-negative or recently tested negative and reported sex with or attraction to men were recruited via either community-based organization (CBO)-mediated local outreach or a national direct-to-consumer (DTC) strategy. Data were collected at baseline and 12 weeks. The primary outcome was a model-based estimate of HIV infections averted per 100 person-years, adjusted for adherent preexposure prophylaxis (aPrEP) use and derived from rectal gonorrhea incidence using a validated predictive model. Implementation costs were assessed using a micro-costing approach. Missing outcome data were addressed using multiple imputation, and sensitivity analyses tested assumptions related to PrEP person-time and model uncertainty.
Study Findings
Direct-to-consumer delivery enrolled a larger proportion of participants overall, whereas CBOs reached a higher share of Black and Latino YMSM. Using imputed data, baseline rectal gonorrhea rates were higher in the CBO arm (5.6% vs 2.7%; P < .001). Engagement, measured by completed intervention modules, was higher in the DTC arm.
Adherent PrEP use increased significantly in both arms at 12 weeks, with a greater increase in the CBO arm (CBO 44.1% vs DTC 27.5%; P < .0001). PrEP-adjusted estimates of HIV infections averted were higher with CBO delivery (1.65/100 person-years; 95% CI, 1.29–2.02) than with DTC delivery (0.62/100 person-years; 95% CI, 0.49–0.74). The cost per HIV infection averted was $983,029 for CBO delivery and $173,313 for DTC delivery, excluding start-up costs.
Clinical Implications
According to the study authors, CBO delivery of KIU! was more effective at reaching YMSM at higher HIV risk and achieving larger short-term gains in PrEP adherence, while the DTC strategy achieved broader reach at substantially lower cost per infection averted. The authors note that public health decision-makers must balance considerations of reach, equity, effectiveness, and cost when selecting implementation strategies for digital HIV prevention interventions.
The authors also highlighted important limitations. Data collection occurred during the COVID-19 pandemic, which disrupted CBO operations and HIV testing access. Outcome data, including sexually transmitted infection testing and follow-up surveys, had substantial missingness and required multiple imputation. Follow-up was limited to 12 weeks, precluding assessment of long-term sustainment. HIV infections were estimated using a predictive model rather than observed seroconversions, and findings may not generalize beyond English-speaking YMSM aged 18–34 years who were not adherent PrEP users at baseline.
Expert Commentary
“These findings contribute valuable insights to guide and improve the future dissemination and implementation of HIV prevention digital health interventions, thereby enhancing scalability, reach, and overall public health impact,” the researchers concluded.
Reference
Mustanski B, Benbow N, Macapagal K, et al. Comparing implementation and effectiveness outcomes for two implementation strategies of the Keep It Up! digital HIV prevention program: a type 3 hybrid effectiveness–implementation trial. AIDS Behav. 2025;29:4030–4042. DOI: 10.1007/s10461-025-04838-0