
Intestinal Lymphangiectasia
{kind=link}
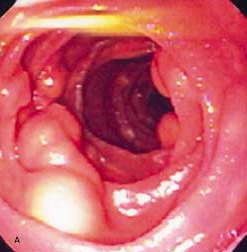 An 81-year-old woman presented with abdominal pain of 6 months’ duration, anorexia, and a 4.5-kg (10-lb) weight loss. Her history was otherwise unremarkable. She denied fever, chills, diarrhea, and vomiting. The pain was diffuse; no rebound or guarding was noted. The peripheral lymph nodes were not palpable. A CT scan revealed multiple para-aortic lymph nodes; no masses were observed in the liver or other organs. An endoscopic evaluation showed multiple white-yellowish, 2-mm to 1-cm nodular lesions in the duodenum that resembled submucosal cysts (A).
An 81-year-old woman presented with abdominal pain of 6 months’ duration, anorexia, and a 4.5-kg (10-lb) weight loss. Her history was otherwise unremarkable. She denied fever, chills, diarrhea, and vomiting. The pain was diffuse; no rebound or guarding was noted. The peripheral lymph nodes were not palpable. A CT scan revealed multiple para-aortic lymph nodes; no masses were observed in the liver or other organs. An endoscopic evaluation showed multiple white-yellowish, 2-mm to 1-cm nodular lesions in the duodenum that resembled submucosal cysts (A).
The nodules were filled with a milk-like fluid that started to flow after biopsy was performed (B). Histopathologic analysis of a biopsy specimen showed an atypical lymphoid infiltrate, which consisted predominantly of B cells. This finding suggested either a reactive process or a low-grade intestinal lymphoma. Laparoscopic biopsy of the para-aortic lymph nodes revealed a high-grade follicular lymphoma. Lucía C. Fry, MD, and Klaus E. Mönkemüller, MD, of Scottsdale, Ariz, write that intestinal lymphangiectasia is the dilatation of intestinal lacteals caused by obstruction of the small intestinal lymphatic system.1
The obstruction can cause rupture of intestinal lymphatics through the mucosa and leakage of lymph into the lumen, which leads to protein-losing enteropathy. Intestinal lymphangiectasia can be congenital or acquired. The primary form, which may be sporadic or familial, occurs in children and in young adults. Secondary intestinal lymphangiectasia usually develops as a consequence of lymph drainage obstruction that results from various conditions, including Whipple disease, mesenteric tuberculosis and sarcoidosis, Crohn disease, lymphenteric fistula, and intestinal lymphoma.2
 In this patient, the lymphoma obstructed the regional lymph nodes, which resulted in the enlargement of the lacteals within the small bowel wall. Large lymphatic cysts thus formed. Biopsy (rupture) of the cysts yielded copious lymph. Secondary intestinal lymphangiectasia can resolve with treatment of the underlying disease. This patient received chemotherapy with cyclophosphamide, vincristine, prednisone, and rituximab. At 6-month follow-up, she was asymptomatic and had gained 6.75 kg (15 lb). Further endoscopic evaluation was unnecessary.
In this patient, the lymphoma obstructed the regional lymph nodes, which resulted in the enlargement of the lacteals within the small bowel wall. Large lymphatic cysts thus formed. Biopsy (rupture) of the cysts yielded copious lymph. Secondary intestinal lymphangiectasia can resolve with treatment of the underlying disease. This patient received chemotherapy with cyclophosphamide, vincristine, prednisone, and rituximab. At 6-month follow-up, she was asymptomatic and had gained 6.75 kg (15 lb). Further endoscopic evaluation was unnecessary.