
Peer Reviewed
Delayed Recognition of Pembrolizumab-Induced Secondary Adrenal Insufficiency
Abstract. This case report discusses an 83-year-old woman with endometrial carcinoma who developed secondary adrenal insufficiency a year after starting pembrolizumab, a PD1 receptor inhibitor. She presented with fatigue and anorexia, with her last infusion two weeks prior. Cortisol studies showed low adrenocorticotropic hormone (ACTH) and cortisol levels. Endocrinology diagnosed secondary adrenal insufficiency due to pembrolizumab, and she was treated with hydrocortisone, which resulted in marked improvement in her symptoms. Although no general recommendations exist for adrenal monitoring for patients prescribed pembrolizumab, adrenal insufficiency should be considered if nonspecific symptoms arise. Measuring endocrine function, including cortisol and ACTH levels, is crucial to detect abnormalities.
Introduction. Immune checkpoint inhibitors (ICI) are monoclonal antibodies used as targeted chemotherapy, approved for use in up to seventeen cancer types. Adverse effects of these medications vary widely depending on organ system and includes endocrinopathies1. With their growing use, the reporting and understanding of associated toxicities has become more common in the literature.
Secondary adrenal insufficiency is a rare but underreported adverse effect of ICIs, such as pembrolizumab, a PD1 receptor inhibitor.1 Adrenal Insufficiency manifests with nonspecific symptoms, including generalized muscle weakness, nausea, and decreased appetite. Symptoms of ICI-induced adrenal insufficiency commonly manifest within 4 to 6 months of treatment initiation.2,3 Due to the potentially life-threatening nature of adrenal insufficiency and possibility of requiring lifelong steroid replacement, the recognition and immediate treatment of adrenal insufficiency is vital for improved patient outcomes.
Previous reports of pembrolizumab-induced adrenal insufficiency detail the commonality of nonspecific presentation and delayed diagnosis, due to various pathophysiological processes.2,4,6 This case illustrates symptomatic secondary adrenal insufficiency with a delayed diagnosis, complicated by cortisol levels that remained within reference range but were progressively declining, initially masking the condition. To our knowledge, no prior reports of pembrolizumab-induced adrenal insufficiency have described a case with a similar clinical presentation or manifestation.
Case Description. We present an 83-year-old woman with a past medical history of hypertension, colonic polyps, diverticulosis, osteopenia, hypothyroidism, and Stage IIIC1 Grade 3 endometrioid endometrial carcinoma diagnosed 13 months before presentation. She was treated with pembrolizumab with adjuvant chemotherapy. She received pembrolizumab therapy for one year, with the last infusion received two weeks before presentation. The patient presented to the hospital with poor oral intake, failure to thrive, hypotension, and delirium. The persistence and worsening of her symptoms prompted the hospital visit. She endorsed symptoms of decreased appetite, weakness, fatigue, dizziness, and lightheadedness during the past 5 months. She denied diarrhea, constipation, urinary symptoms, or chest pain. At the time of presentation, her medications included 20 mg atorvastatin, 100 mg thiamine, 37.5 mcg levothyroxine, and 50 mg tramadol. Laboratory testing revealed elevated inflammatory markers, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP).
Differential diagnoses included hypothyroidism, metabolic abnormalities, and pembrolizumab-induced adverse effects. These were considered due to her past medical history of hypothyroidism, recent initiation of chemotherapy, and consideration of common causes of delirium in an elderly patient. An extensive workup was conducted to address these differentials. The following morning, diagnostic workup revealed low cortisol AM level at 0.2 (normal range, 4.8-19.5 ug/dL) and ACTH at 2.4 (normal range, 7.2-63.3 pg/dL). Additionally, complete blood count, thyroid-stimulating hormone, magnesium, phosphorus, B-vitamins, folate and creatine kinase were within normal limits. ACTH was collected again the next morning with persistently low levels at 1.7. Endocrinology was consulted, and the final diagnosis of secondary adrenal insufficiency due to pembrolizumab was confirmed as all other causes were ruled out.
On recommendation of endocrinology, the patient started high-dose hydrocortisone 30 mg twice daily during her three-day hospital stay. She was noted to have significant improvement within her hospital stay, such as an increase in appetite, restoration of baseline blood pressure, and increased activity tolerance. She was discharged with a tapering schedule of hydrocortisone to 10 mg every morning and 5 mg every evening. On subsequent gynecology-oncology follow-up one month later, cortisol levels returned to reference range and the patient endorsed cessation of her previous symptoms, including increased appetite and energy levels. She remains on a maintenance dose of 15 mg hydrocortisone daily. In our case, patient outcome and follow-up revealed adequate treatment and resolution of symptoms.
Discussion. Pembrolizumab is an ICI targeting PD-1 on T-Cells, inhibiting cancer cells from suppressing the immune system response. Pembrolizumab has been FDA approved for the treatment of several cancer types, including endometrial carcinoma. Endocrinopathies are known adverse effects of ICIs, including thyroid and adrenal disorders. Adrenal insufficiency is uncommon, with a documented incidence of approximately 1%.4 The rarity of this adverse event, combined with its nonspecific presentation, complicates timely diagnosis and attributing the etiology to pembrolizumab.
Adrenal insufficiency is the inability of the adrenal cortex to sufficiently maintain the production and secretion of glucocorticoids and/or mineralocorticoids, which play a vital role in the body’s homeostasis of salt, energy, and fluids. The deficiency of these hormones is a potentially life-threatening condition, which requires prompt diagnosis and treatment via cortisol replacement therapy. Symptom presentation is largely nonspecific, with common manifestations including fatigue, anorexia, weight loss, lightheadedness, and dizziness. The diagnosis of adrenal insufficiency begins with morning cortisol levels < 5 ug/dL followed by a Cosyntropin Stimulation Test, where a cortisol level < 18 ug/dL is consistent with adrenal insufficiency.5
The mechanism behind pembrolizumab-induced adrenal insufficiency is not clearly understood but is commonly attributed to hypophysitis, which presents with both ACTH and cortisol deficiencies.6 This mechanism is similar to hypophysitis induced by another ICI, ipilimumab, with features of both AI and hypothyroidism. Our patient's low ACTH and cortisol levels are likely attributable to hypophysitis, although the underlying cause remains uncertain. Our patient’s delayed diagnosis leading to her hospitalization was likely due to normal cortisol levels, which initially masked the condition (Table 1). The onset of her symptoms began 9 months after the initial infusion of pembrolizumab with stable cortisol levels.
Table 1. Morning cortisol trends
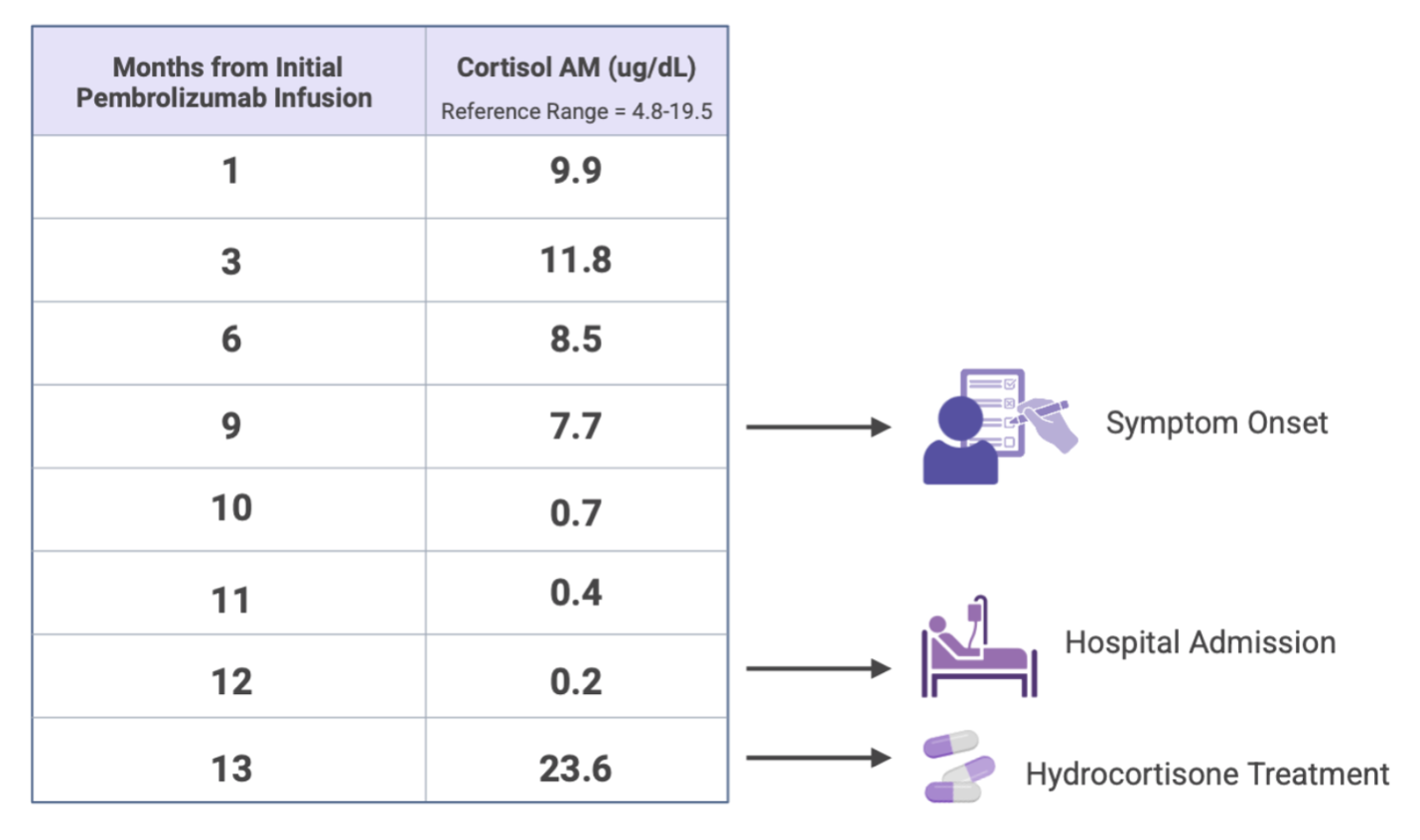 Our case was unique in that the patient was symptomatic despite initial cortisol levels falling within normal ranges, with a decline that revealed the diagnosis after hospitalization. Upon literature review, previous case reports detail adrenal insufficiency after cessation of treatment but with different features from our patient’s presentation, such as varying times of presentation after cessation of pembrolizumab (10 days to 8 months), additional secondary hypothyroidism, ketosis, hypertension, or pancytopenia .2,4,6 To mitigate the likelihood of hospitalization, we recommend maintaining a high index of clinical suspicion in symptomatic patients, with close monitoring and scheduled follow-up of cortisol levels in those receiving pembrolizumab therapy.
Our case was unique in that the patient was symptomatic despite initial cortisol levels falling within normal ranges, with a decline that revealed the diagnosis after hospitalization. Upon literature review, previous case reports detail adrenal insufficiency after cessation of treatment but with different features from our patient’s presentation, such as varying times of presentation after cessation of pembrolizumab (10 days to 8 months), additional secondary hypothyroidism, ketosis, hypertension, or pancytopenia .2,4,6 To mitigate the likelihood of hospitalization, we recommend maintaining a high index of clinical suspicion in symptomatic patients, with close monitoring and scheduled follow-up of cortisol levels in those receiving pembrolizumab therapy.
Conclusion. This case emphasizes the importance of being vigilant for adrenal insufficiency in patients receiving treatment with ICIs such as pembrolizumab. Even when cortisol levels are within normal range, clinicians should consider adrenal insufficiency if ACTH levels are low, and the patient is showing unspecific symptoms like fatigue and decreased appetite. A multidisciplinary team approach involving oncologists, endocrinologists, and primary care doctors is essential for prompt diagnosis and management of this rare but serious condition. Additional research is needed to improve diagnostic methods and treatment strategies for endocrinopathies caused by ICIs.
AUTHORS:
Lyiba Malik, MS1 • Asil Habash, MD2 • Ellen Schmitt, MD3
AFFILIATIONS:
1Medical College of Wisconsin, Milwaukee, WI
2Department of Family Medicine, Medical College of Wisconsin, Milwaukee, WI
3Department of Geriatrics and Palliative Care, Medical College of Wisconsin, Milwaukee, WI
CITATION:
Malik L, Habash A, Schmitt E. Delayed recognition of pembrolizumab-induced secondary adrenal insufficiency: A case report. Consultant. Published online November 5, 2025. DOI: 10.25270/con.2025.11.000001
Received June 9 2025. Accepted July 22, 2025.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE:
Lyiba Malik, MS, 8701 W Watertown Plank Rd, Milwaukee, WI (lmalik@mcw.edu)
References
- Wright JJ, Powers AC, Johnson DB. Endocrine toxicities of immune checkpoint inhibitors. Nat Rev Endocrinol. 2021;17(7):389-399. doi:10.1038/s41574-021-00484-3
- Escaño L, Desai P. Secondary adrenal insufficiency as an immune-related adverse event of pembrolizumab therapy. Cureus. 2024;16(7):e65163. doi:10.7759/cureus.65163
- Grouthier V, Lebrun-Vignes B, Moey M, et al. Immune checkpoint inhibitor-associated primary adrenal insufficiency: WHO VigiBase report analysis. Oncologist. 2020;25(8):696-701. doi:10.1634/theoncologist.2019-0555
- Zilberman S, Rafii DC, Giunta J. Pembrolizumab-induced adrenal insufficiency presenting eight months after cessation of treatment. Cureus. 2023;15(6):e41049. doi:10.7759/cureus.41049
- Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and treatment of primary adrenal insufficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2016;101(2):364-389. doi:10.1210/jc.2015-1710
- Doodnauth AV, Klar M, Mulatu YS, et al. Pembrolizumab-induced hypophysitis with isolated adrenocorticotropic hormone (ACTH) deficiency: a rare immune-mediated adverse event. Cureus. 2021;13(6):e15465. doi:10.7759/cureus.15465