
Prevention and Prophylaxis of Malaria in Older Travelers
At the conclusion of this activity, participants should be able to:
1. Recognize the need for malaria prophylaxis in older adults who are planning international travel.
2. Identify common and uncommon adverse effects of antimalarial agents.
3. Describe common drug interactions among antimalarial agents and medications commonly used in older adults.
4. Identify important contraindications to specific malaria prophylaxis regimens.
_________________________________________________________________________________________________________________________
INTRODUCTION
The prevention of malaria is an essential part of vacation planning for those traveling to areas of the world where malaria is endemic, especially among older adults who are at increased risk of complications related to infection. Preventive measures fall into two equally important categories: the first focuses on decreasing exposure to potentially infectious mosquitoes; the second involves administration of low-dose antimicrobial drugs for “chemoprophylaxis” against infection. In the following review, we will address these issues with the older traveler in mind.
OVERVIEW OF MALARIA
Human malaria results from infection with one of four species of the Plasmodium parasite: P. falciparum, P. vivax, P. ovale, and P. malariae. In regions of the world where human malaria is endemic, Plasmodium infection is transmitted to humans by the female Anopheles mosquito, which generally feeds (and thus transmits malaria) between sunset and sunrise, with the highest activity during dusk and dawn. Travelers must remember that in malariaendemic regions, other mosquito species as well as other biting insects must also be avoided. In addition to malaria, insects transmit dengue fever, chikungunya fever (both spread by the Aedes mosquito), and leishmaniasis (transmitted by sand flies). Unlike the Anopheles mosquito, Aedes mosquitoes feed during the daytime, which is why “around-theclock” insect protection is vital.
Like many serious infections, malaria has a more severe presentation in older adults. Compared to younger patients, older travelers with malaria can expect to have higher death rates, higher levels of parasitemia, more complications, and protracted illness.1-3 Age-related immune senescence, underlying comorbid conditions, and higher susceptibility to the negative effects of cytokines during acute infection are felt, in part, to be responsible for worse outcomes. For these reasons, disease prevention is important for safe travel among older adults.
THE BASICS OF MOSQUITO AVOIDANCE
 Mosquito avoidance is a fundamental aspect of malaria prevention. Basic interventions such as bed nets, proper clothing, and effective repellents can help decrease the risk of malaria significantly (Table I). Simply put, if you don’t get bitten, you won’t get malaria or other insect-borne infections.
Mosquito avoidance is a fundamental aspect of malaria prevention. Basic interventions such as bed nets, proper clothing, and effective repellents can help decrease the risk of malaria significantly (Table I). Simply put, if you don’t get bitten, you won’t get malaria or other insect-borne infections.
Mosquito bed nets come in a variety of shapes and sizes, and can be free-standing (used mainly for camping) or hung from the ceiling over the bed (a more permanent arrangement). Nets are more effective when impregnated with an insecticide such as permethrin (see below). The mesh that makes up the net should have holes that measure no larger than 1.5 mm.4 If the free-standing mosquito net has an open bottom, care should be taken to arrange bedding so that no access is available for mosquitoes or other insects to enter. Pieces of wadded tissue paper can help seal off holes in the mesh if they are present.
Clothing, another important adjunct to mosquito protection, should protect as much exposed skin as comfortably possible. Longsleeved shirts and long pants will help serve as a barrier to mosquito bites in high-risk areas. Application of permethrin to clothing will further decrease this risk. Pants should be tucked into socks or hiking boots to help protect this vulnerable area from insect bites.
Mosquito Repellents
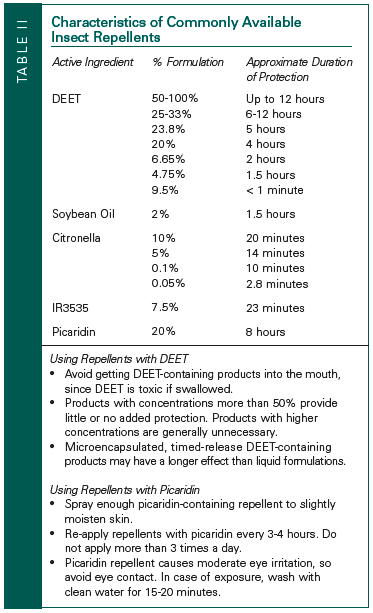 There are a myriad of insect repellents available to the traveler, ranging from synthetic to organic formulations (Table II). Despite popular opinion and advertising, many products have limited, if any, efficacy. The most thoroughly researched and proven insect repellent available contains N, N-diethyl-m-toluamide, also known as DEET.5,6 A single application of a 50% DEET-containing formulation provides up to 12 hours of protection. Although highly effective, DEET can damage synthetic clothing and eyewear containing plastic components, and can leave behind an oily residue that is unpleasant for some users.
There are a myriad of insect repellents available to the traveler, ranging from synthetic to organic formulations (Table II). Despite popular opinion and advertising, many products have limited, if any, efficacy. The most thoroughly researched and proven insect repellent available contains N, N-diethyl-m-toluamide, also known as DEET.5,6 A single application of a 50% DEET-containing formulation provides up to 12 hours of protection. Although highly effective, DEET can damage synthetic clothing and eyewear containing plastic components, and can leave behind an oily residue that is unpleasant for some users.
An alternative insect repellent, picaridin, which has been available for years in Australia and Europe in a 20% formulation, recently became available in the United States in both a 7% and 15% formulation.7 The 20% formulation available outside the United States provides up to 8 hours of protection after an application. Due to the limited data on protection time for concentrations of picaridin available in the United States, re-application every 3-4 hours is recommended. Despite the need for more frequent application, picaridin does not feel greasy and does not damage clothing or eyeglasses, and may be more acceptable to those who find DEET unpleasant. No serious reactions have been reported in humans from use of picaridin in Australia and Europe.7
Most other available formulations of insect repellents, including those with citronella, eucalyptus oil, alanine analogs (bath oil), and soybean oil, do not provide adequate protection against mosquitoes for travelers.8 Permethrin, an insecticide commonly used as a treatment for lice, is available in a spray formulation. Permethrin is not designed to be sprayed onto the skin, but rather to be applied to clothing, bed nets, tents, and sleeping bags, providing additional protection against mosquitoes. Although permethrin acts as a neurotoxin for insects, this agent is poorly absorbed and safe for humans. Permethrin is odorless, non-staining, and resistant to degradation by light, heat, and immersion in water. Insect repellent effects of permethrin can persist even after multiple washings.6
MALARIA CHEMOPROPHYLAXIS
Chemoprophylaxis, the other essential component of malaria prevention, is recommended during travel to a malaria-endemic region for more than a few days. Specific chemoprophylaxis regimens should be selected carefully, taking into consideration the perspective traveler’s medical history and concurrent medications. As much as possible, the regimen should be well tolerated, simple to administer, and have minimal side effects and drug interactions. Below, we review the major drugs currently available for malaria chemoprophylaxis. While drug-drug interactions exist with each of these agents, many of these interactions are only clinically important at higher treatment doses, as opposed to the lower doses used for chemoprophylaxis. However, understanding these potential interactions along with the associated side effects will help healthcare providers choose the optimal regimen for each traveler (Table III).

Chloroquine
Chloroquine remains the first-line agent for chemoprophylaxis for travelers visiting areas where chloroquine-resistant strains of malaria do not exist, which is now limited to some parts of the Caribbean and Central America. Because of high levels of resistance throughout the vast majority of malaria-endemic regions, chloroquine holds very limited utility as prophylaxis.
 Chloroquine is available as either chloroquine phosphate or hydroxychloroquine sulfate. Chloroquine phosphate is available as a 500-mg tablet (300-mg base) and hydroxychloroquine sulfate as a 400-mg tablet (310-mg base). For malaria chemoprophylaxis, either formulation should be taken orally once weekly beginning 2 weeks prior to travel, continued weekly throughout the stay, and continued for 4 additional weeks after departure from the region.
Chloroquine is available as either chloroquine phosphate or hydroxychloroquine sulfate. Chloroquine phosphate is available as a 500-mg tablet (300-mg base) and hydroxychloroquine sulfate as a 400-mg tablet (310-mg base). For malaria chemoprophylaxis, either formulation should be taken orally once weekly beginning 2 weeks prior to travel, continued weekly throughout the stay, and continued for 4 additional weeks after departure from the region.
Except for its bitter taste, chloroquine is usually well tolerated. A nonallergic, generalized pruritis in individuals of African descent has been described.9 Older travelers with renal insufficiency (creatinine clearance < 10 mL/min) should be given 50% of the recommended dose (150-mg chloroquine phosphate base or 155-mg hydroxychloroquine sulfate base) (Table IV). Minor side effects associated with chloroquine include gastrointestinal disturbances, dizziness, blurred vision, and headache. Retinal injury secondary to chloroquine is described in association with higher doses used to treat rheumatoid arthritis. However, if a traveler has baseline retinal pathology, it may be prudent to select an alternative chemoprophylaxis regimen. Chloroquine should also be used with caution in elderly travelers with blood dyscrasias, psoriasis, porphyria, liver disease, and heavy alcohol consumption.
Important drug interactions may result with antiarrhythmics, antiemetics (including scopolamine), tricyclic antidepressants, selective serotonin reuptake inhibitors, as well as fluconazole, fluoroquinolones, and macrolides, all of which may result in QT prolongation, torsades de pointes, and/or cardiac arrest. While these adverse effects are rarely seen with prophylactic doses of chloroquine, it is important to consider these potential interactions when determining an appropriate regimen.
Mefloquine
Mefloquine is active against many chloroquineresistant and sulfadoxine/pyrimethamine-resistant malaria strains, resulting in a much wider geographic utility for prophylaxis. Mefloquine, however, cannot be used where mefloquineresistant strains of P. falciparum have been documented, most notably the forested areas along the borders of Thailand with both Cambodia and Myanmar. Alternative agents effective against mefloquine-resistant P. falciparum (atovaquone/proguanil or doxycycline) should be used if travelers are planning to be in these regions. In 2003, the Centers for Disease Control and Prevention reported 54 cases of proven P. falciparum malaria among U.S. civilians. Compliance with malaria chemoprophylaxis was documented in 14 (26%) of these cases, with 13 of the individuals using mefloquine as their chemoprophylactic agent. All 14 of these patients had traveled to Africa, which raises concern of a trend toward mefloquine failure in Africa, and must be considered when using this drug.10
Mefloquine is generally given as a 250-mg tablet weekly starting 1-2 weeks prior to travel into the endemic region, continued weekly during travel, and then for 4 additional weeks after return from the endemic area. For those traveling at the last minute to a malaria-endemic region who are unable to begin chemoprophylaxis 2 weeks prior to travel, a loading dose of 250 mg orally daily for 3 days is recommended prior to starting the weekly schedule.
Mefloquine should not be used in patients with a history of psychiatric illness or severe depression. Side effects such as lightheadedness, bad dreams, paranoid ideation, seizures, and psychosis have been reported with mefloquine. However, when studied closely, the incidence of these side effects was comparable to that seen with chloroquine use.11 Other common side effects with mefloquine include dizziness, diarrhea, nausea, vomiting, and somnolence. Fortunately, approximately 40% of adverse events will occur following the first dose, and nearly 80% will have occurred by the third dose.12 Therefore, if concern exists over whether mefloquine will be tolerated by a patient, prophylaxis with the drug may be initiated several weeks prior to departure to determine patient tolerance.
Potential drug interactions that may occur in older patients include those with antiarrhythmics, propranolol, quetiapine, antiemetics, azoles, rifampin, and macrolides that may potentially result in QT prolongation and/or torsades de pointes. These interactions have largely been theoretical and in a statement regarding the safety of mefloquine in malaria prophylaxis, the World Health Organization considers mefloquine, in prophylactic doses, safe to use with most of these medications.13 Patients taking rifampin, rifabutin, or tetracycline will have decreased blood levels of mefloquine, and may place patients at increased risk of contracting malaria. Mefloquine may also increase metabolism of valproic acid, potentially placing a patient with wellcontrolled seizures at risk for seizures.
Atovaquone/Proguanil
Fixed-dose combination atovaquone/proguanil is well tolerated and convenient, making it a commonly prescribed agent for malaria prophylaxis. The effectiveness of atovaquone/proguanil against chloroquine-resistant and mefloquine-resistant P. falciparum also makes it an attractive option in areas where multidrug-resistant P. falciparum is endemic. Recently, new concerns for atovaquone/proguanil resistance among P. falciparum have been raised with the identification of specific mutations on the cytochrome b gene of P. falciparum in Nigeria. This highlights concerns about emerging resistance of P. falciparum to atovaquone/proguanil14 and underscores the fundamental importance of mosquito avoidance along with appropriate follow-up of febrile illness in returning travelers.
The adult formulation of atovaquone/proguanil comes in a fixed-dose combination of atovaquone 250 mg plus proguanil hydrochloride 100 mg in a single tablet. Dosing for malaria chemoprophylaxis is 1 tablet by mouth daily starting 1-2 days prior to malaria exposure and continuing for 1 week after departure from the endemic region. Atovaquone/proguanil is contraindicated in patients with creatinine clearance < 30 mL/min. In addition, atovaquone/proguanil rarely can cause neutropenia and pancytopenia, and therefore should not be used in patients with a history of blood dyscrasias.
While atovaquone/proguanil is generally well tolerated, minor side effects such as abdominal pain, nausea, vomiting, headache, and rash are frequent.15 The weekly cost of atovaquone/proguanil is higher than other regimens, so prolonged use may not be practical (Table V). Another potential disadvantage of atovaquone/proguanil is the need for daily administration. Any lapses in adherence with malaria chemoprophylactic medications place the traveler at risk, especially when dealing with agents requiring daily administration due to their shorter half-life.

Important drugs that potentially interact with either component of atovaquone/proguanil include warfarin, tetracycline, rifampin, and the oral typhoid vaccine. Rifampin and tetracycline will decrease the concentration of atovaquone in serum. Coagulation parameters should be monitored closely in patients on warfarin, as proguanil may increase anticoagulation effect. Finally, proguanil may decrease immune response to the oral (live) typhoid vaccine. Therefore, a 10-day period should be allowed after the last dose of oral typhoid vaccine and the administration of atovaquone/proguanil.
Doxycycline
Doxycycline is effective for chemoprophylaxis in regions where chloroquine-resistant, mefloquineresistant, and sulfadoxine/pyrimethamine-resistant malaria are endemic,16 and may also provide prophylaxis against leptospirosis and rickettsial infections.17 These characteristics, in addition to low cost and relatively few drug interactions, make doxycycline an attractive choice for malaria prophylaxis. However, the need for daily administration, high risk of photosensitivity, and potential for pill esophagitis are notable downsides to this agent.
The risk of photosensitivity with doxycycline, especially in tropical areas, is problematic, and cutaneous reactions can be quite severe. Unfortunately, sunscreens do not block ultraviolet A rays well enough to completely prevent these reactions. The older traveler who will likely have significant sun exposure during travel should not use doxycycline as first-line malaria chemoprophylaxis. If doxycycline is used, sun exposure should be minimized using large-brimmed hats, long-sleeved shirts and pants, ultraviolet protection factor–rated clothing, and sunscreen protection with UVA and UVB protection. The risk of pill esophagitis from doxycycline can be reduced by taking pills with adequate amounts of water.
The dose for doxycycline as malaria chemoprophylaxis is 100 mg daily beginning 1-2 weeks prior to entrance into endemic region and continuing for 4 weeks after return. If patients are taking minocycline for the treatment of rheumatoid arthritis, and an alternative chemoprophylactic agent cannot be used, then the doxycycline should replace minocycline during travel, as the efficacy of minocycline has not been established in malaria prophylaxis.
Despite the low dose of doxycycline used for malaria prophylaxis, older travelers on concurrent digoxin, methotrexate, rifampin, and warfarin may need monitoring. Doxycycline can increase methotrexate levels and potentially exacerbate methotrexate toxicity (bone marrow suppression, nephrotoxicity, mucosal ulcerations). In addition, doxycycline can increase digoxin levels and increase risk of bleeding in patients taking warfarin. Patients taking rifampin will have lower doxycycline concentrations in their plasma, placing them at risk for drug failure.
Sulfadoxine/Pyrimethamine
Sulfadoxine/pyrimethamine is not recommended for malaria prophylaxis for U.S. travelers. Severe mucocutaneous reactions, including erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal necrolysis have been described after two or more doses of sulfadoxine/pyrimethamine. These reactions produced fatalities at a rate of about 1/11,000 to 20,000 among U.S. travelers, thus limiting the utility of this agent.18
Primaquine
In general, primaquine is reserved for travelers with potential heavy exposure to P. vivax or P. ovale, although the ideal use of primaquine in prevention remains unclear. If used as prophylaxis, 30 mg (base) orally is given once daily, beginning 1 day before departure, and continuing for 7 days after leaving the malarious area. Although the role in prophylaxis is limited, primaquine is frequently used to treat actual malaria infection.
When used to treat infection of P. vivax and P. ovale, primaquine eradicates the persistent hepatic stages of the parasite (hypnozoite) which, when present, can cause persistent relapses for up to 4 years after routine treatment. Some physicians will administer a course of primaquine during the last week of or just after a course of malaria prophylaxis with chloroquine, mefloquine, atovaquone/proguanil, or doxycycline. If used in this way, primaquine may be administered as 15 mg of the base daily for 14 days or as 45 mg of the base once per week for 8 weeks.
Common side effects of primaquine include gastrointestinal upset, sometimes necessitating discontinuation of the medication. Primaquine is contraindicated in patients with lupus erythematosus and rheumatoid arthritis. This agent can cause hemolytic anemia in patients with glucose- 6-phosphate dehydrogenase (G6PD) deficiency, which must be ruled out prior to administration.
Proguanil
While not available in the United States, proguanil is available in Canada, Europe, and much of Africa. Proguanil is a dihydrofolate reductase inhibitor like the pyrimethamine component of sulfadoxine/pyrimethamine. If used as prophylaxis, the dose administered should be 200 mg orally each day and should be taken in combination with chloroquine. However, as proguanil is not readily available in the United States and the combination of chloroquine/proguanil has been shown to be less effective against P. falciparum than mefloquine, this combination is not recommended often.11,19,20 As with atovaquone/proguanil, the proguanil component of chloroquine/proguanil interacts with warfarin and efficacy of the typhoid vaccine (see above).
SUMMARY
The serious and potentially fatal consequences of malaria in the older traveler, coupled with emerging resistance in many areas around the world, make malaria chemoprophylaxis and education on mosquito avoidance very important priorities for the physician. It is important to know that no mosquito prophylaxis regimen is 100% effective, and that patient education, symptom surveillance, and close follow-up should be available to all returning travelers.
The older traveler should be aware of the symptoms of malaria and understand that they can occur anywhere from weeks (in the case of P. falciparum) to a few months and even years (in the cases of P. vivax and P. ovale) after return. The development of fevers, chills, myalgias, or gastrointestinal complaints should prompt an older adult to visit his or her healthcare provider. Finally, consultation with a Travel Medicine specialist should be sought several months prior to international travel to allow adequate time for trip planning, appropriate vaccinations, and monitoring of adverse effects or interactions of chosen malaria chemoprophylactic regimens. With a bit of simple, common sense planning and preventive measures, older adults can decrease the risk of malaria—and focus on enjoying their travels fully.
The research reported in this article is supported by the John A. Hartford Foundation Center of Excellence in Geriatrics and the Veterans Affairs Ann Arbor Healthcare System Geriatric Research, Education, and Clinical Center (GRECC).
1. Schwartz E, Sadetzki S, Murad H, Raveh D. Age as a risk factor for severe Plasmodium falciparum malaria in nonimmune patients. Clin Infect Dis 2001;33:1774-1777. Epub 2001 Oct 12.
2. Gjørup IE, Rønn A. Malaria in elderly nonimmune travelers. J Travel Med 2002;9:91-93.
3. Jensenius M, Rønning EJ, Blystad M, et al. Low frequency of complications in imported falciparum malaria: A review of 222 cases in south-eastern Norway. Scand J Infect Dis 1999;31:73-78.
4. World Health Organization. Environmental health risks. International Travel and Health 2007; World Health Organization; 2007:30-48. Available at: www.who.int/ith/en/. Accessed June 14, 2007.
5. Insect repellents. The Medical Letter on Drugs and Therapeutics 2003;45(1157):41-44.
6. Gupta RK, Rutledge LC. Laboratory evaluation of controlledrelease repellent formulations on human volunteers under three climatic regimens. J Am Mosq Control Assoc 1989;5:52-55.
7. Picaridin—A new insect repellent. The Medical Letter on Drugs and Therapeutics 2005;47(1210):45-48.
8. Fradin MS, Day JF. Comparative efficacy of insect repellents against mosquito bites. N Engl J Med 2002;347:13-18.
9. Salako LA. Toxicity and side-effects of antimalarials in Africa: A critical review. Bull World Health Organ 1984;(62 suppl): 63-68.
10. Eliades JM, Shah S, Nguyen-Dinh P, et al. Malaria surveillance— United States, 2003. MMWR Surveill Summ 2005;54(2):25-40.
11. Steffen R, Fuchs E, Schildknecht J, et al. Mefloquine compared with other malaria chemoprophylactic regimens in tourists visiting east Africa. Lancet 1993;341:1299-1303.
12. Stürchler D, Handschin J, Kaiser D, et al. Neuropsychiatric side effects of mefloquine. New Engl J Med 1990;322:1752- 1753.
13. World Health Organization: Mefloquine: Update on safety issues. WHO Drug Info 1996;10:58-61.
14. Happi CT, Gbotosho GO, Folarin OA, et al. Confirmation of emergence of mutations associated with atovaquone/ proguanil resistance in unexposed Plasmodium falciparum isolates from Africa. Malar J 2006;5:82.
15. Camus D, Djossou F, Schilthuis HJ, et al. Atovaquoneproguanil versus chloroquine-proguanil for malaria prophylaxis in nonimmune pediatric travelers: Results of an international, randomized, open-label study. Clin Infect Dis 2004;38:1716-1723. Epub 2004 May 27.
16. Centers for Disease Control and Prevention. Travelers’ Health: Yello Book. Health Information for International Travel, 2005-2006. DHHS, Atlanta, GA, 2001. Available at: www.cdc.gov/travel/yb/. Accessed June 15, 2007. 17. Magill AJ. The prevention of malaria. Prim Care 2002;29:815-842.
18. Centers for Disease Control (CDC). Adverse reactions to Fansidar and updated recommendations for its use in the prevention of malaria. MMWR Morb Mortal Wkly Rep 1985;33(51-52):713-714.
19. Weiss WR, Oloo AJ, Johnson A, et al. Daily primaquine is effective for prophylaxis against falciparum malaria in Kenya: Comparison with mefloquine, doxycycline, and chloroquine plus proguanil. J Infect Dis 1995;171:1569-1575.
20. Barnes AJ, Ong EL, Dunbar EM, et al. Failure of chloroquine and proguanil prophylaxis in travellers to Kenya. Lancet 1991;338:1338-1339.