
Heat-Related Illness in the Elderly
At the conclusion of this activity, participants should be able to:
1. Identify physiologic changes with aging that predispose the elderly to heatrelated illnesses.
2. Identify risk factors associated with heat-related illnesses in older adults.
3. Accurately diagnose and differentiate the common forms of minor heatrelated illnesses (heat cramps, heat edema, head syncope, and prickly heat).
4. Differentiate the presentation and treatment of heat exhaustion and heat stroke in the elderly.
5. Recommend pharmacologic treatment and manage miscellaneous concerns, including pulmonary rehabilitation, surgery, smoking cessation, and immunizations for stable COPD.
_________________________________________________________________________________________________________________________
INTRODUCTION
Summer heat waves are among the deadliest environmental events, often accompanied by stories of heat-related deaths, usually involving the elderly. In the United States, an average of 400 Americans die each year from excessive heat. Last summer, newspaper headlines in the Southwest described the problem concisely. For example, the Los Angeles Times declared “Elderly, Isolated Are Heat’s Quiet Victims” after a week-long unprecedented heat wave in California that resulted in the deaths of 72 people.1 In the summer of 2003, August temperatures in France reached unexpected and unprecedented highs, resulting in the deaths of more than 10,000 people. The largest single heatrelated disaster occurred in 1995 when an extreme heat wave in Chicago resulted in more than 700 deaths. The elderly and those who live alone or are unable to care for themselves represent the vast majority of these heat-related deaths. Thus, at-risk individuals can be readily identified and could be targets of effective preventive strategies. This article reviews the pathophysiology of heat regulation; the medical, environmental, and social components of heat-related illness in the elderly population; and the essential elements of early identification and proper treatment of these conditions.
PATHOPHYSIOLOGY
Hyperthermia is an increase in body temperature due to an imbalance between heat production and dissipation. It also describes a group of heat-related emergencies in which the hypothalamus fails to regulate the balance between heat dissipation and heat accumulation. This failure may manifest itself as minor ailments such as heat cramps or heat edema, or as the more serious, life-threatening condition of heat stroke.
Decreased heat dissipation occurs with age due to a decline in lean body mass (greater barrier to heat exchange) and reduced superficial microvasculature (decreased circulation to cooler external body surfaces). Evaporation accounts for 20-30% of heat loss at rest and essentially all heat loss at air temperatures above 95 degrees F. Significant atrophy of sweat glands in the elderly makes heat dissipation by evaporation far less effective.2
The physiologic basis of thermoregulation is not completely understood. Current understanding is that homeostatic temperature control is maintained by a triad of thermosensors, a central integrative area, and thermoregulatory effectors. Thermosensors are temperature-sensitive collections of specialized neurons located peripherally in skin and centrally in the preoptic area of the anterior hypothalamus and the spinal cord that interpret changes in body temperature and regulate heatdissipating responses.3 With increasing age, individual thermosensors, both central and peripheral, become less effective in responding to temperature changes. Whether this is due to a decrease in sensitivity or in overall number is unknown, but the effect is the same: a decreased perception of heat in the elderly with associated reduction in heat-dissipation mechanisms.
It is unclear whether the setpoint that keeps body temperature within a narrow range is a property of a specific autonomic structure within the central nervous system (CNS) or the result of a complex system lacking a central control center.4 Evidence suggests the existence of a central integrative mechanism at the hypothalamic or spinal cord level.
Thermoregulatory effectors are physiologic mechanisms that accelerate heat loss and are triggered by thermosensors via the central integrative area. The two primary effectors are sweat production and peripheral vasodilatation. In a warm environment, evaporation of sweat from the skin is the most important mechanism of heat dissipation. Heat loss from the skin by convection and radiation is maximized by increased skin blood flow, which also carries heat convectively from the core to the surface.5 Of the triad, thermoregulatory effectors are the most likely to become compromised by the aging process due to the increased incidence of skin and vascular disease in the elderly.
RISK FACTORS FOR HEAT ILLNESS
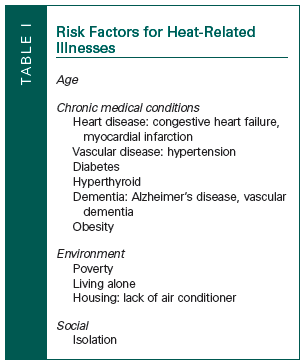 Heat illness can be divided into two distinct types: exertional and sedentary. The elderly are at increased risk for both, although the sedentary type predominates in this population. Age is a risk factor for heat-related illness due to compromised heat-dissipation and regulation mechanisms as described above, but these are not the only factors that explain age-related susceptibility.6 Other factors associated with increased risk for heat illness in the elderly are chronic medical conditions, social circumstances, medication use, environment, mental impairment, and physical impairment or bed confinement—circumstances that interfere with the ability to care for oneself or to avoid hot environments (Table I).7
Heat illness can be divided into two distinct types: exertional and sedentary. The elderly are at increased risk for both, although the sedentary type predominates in this population. Age is a risk factor for heat-related illness due to compromised heat-dissipation and regulation mechanisms as described above, but these are not the only factors that explain age-related susceptibility.6 Other factors associated with increased risk for heat illness in the elderly are chronic medical conditions, social circumstances, medication use, environment, mental impairment, and physical impairment or bed confinement—circumstances that interfere with the ability to care for oneself or to avoid hot environments (Table I).7
Chronic Medical Conditions
Chronic medical conditions significantly alter the body’s physiologic response to heat load or the ability to tolerate changes in core body temperature. Cardiovascular disease is the most significant condition that predisposes to heat illness. Cardiac disease that reduces cardiac output, such as heart failure and myocardial infarction, may also impair cutaneous vasodilatation. Vascular disease reduces the effective circulation of blood to the cutaneous beds. Chronic conditions such as atherosclerosis, hypertension, and diabetes mellitus all decrease vascular compliance, thus reducing effective cooling measures and can culminate in vascular collapse with seemingly minor shifts in volume status.
Other chronic conditions that increase risk for heat-related illness are hyperthyroidism, psychiatric disorders, and extensive skin disease or damage. Hyperthyroidism, through excess secretion of thyroid hormone, produces a hypermetabolic state that can lead to hyperpyrexia. Psychiatric disorders, such as delirium and dementia, impair cognitive abilities to both perceive heat and the initiation to take steps to reduce heat stress. Skin disease, such as scleroderma and ectodermal dysplasia, reduce heat dissipation by physiologically changing the skin into a nonpermeable barrier.
Obesity, which affects an estimated 33% of the population age 65 years or older, is another risk factor for heat-related illness.8 Increased body mass means more heat generated for the same level of activity and leads to less efficient heat dissipation. Adipose tissue acts as insulation, and fewer heatactivated sweat glands are found in skin overlying adipose tissue. Obesity also causes decreased cardiac output per unit of body weight, thus hampering the cardiac role in heat dissipation.
Dehydration alone can produce hyperthermia, as well as be a contributing factor to heat-related illness. The decline in total body water, the decreased ability to concentrate urine, and the diminished sensation of thirst that occurs with age places older individual at increased risk for dehydration. Gastrointestinal absorption of fluids decreases with age, compounding the risk of predisposition to dehydration among the elderly. Dehydration and the subsequent hyperosmolarity it produces decreases sweat production, further reducing the effectiveness of this heat loss mechanism.
 The elderly are high consumers of medications, responsible for 34% of prescription drugs and 40% of all over-the-counter medications.9,10 Certain classes of medications predispose older adults to heat-related illness (Table II). Drugs commonly prescribed for hypertension, such as beta blockers and calcium channel blockers, reduce vascular compliance for heat-dissipation mechanisms. Diuretics, also commonly used for hypertension and for heart disease, reduce fluid volume, leading to dehydration. Anticholinergic agents, such as those used for Parkinson’s disease, decrease sweat production.
The elderly are high consumers of medications, responsible for 34% of prescription drugs and 40% of all over-the-counter medications.9,10 Certain classes of medications predispose older adults to heat-related illness (Table II). Drugs commonly prescribed for hypertension, such as beta blockers and calcium channel blockers, reduce vascular compliance for heat-dissipation mechanisms. Diuretics, also commonly used for hypertension and for heart disease, reduce fluid volume, leading to dehydration. Anticholinergic agents, such as those used for Parkinson’s disease, decrease sweat production.
Environmental and Social Risk Factors
Environment and lack of social support systems are two significant, often overlooked factors regarding the elderly and heat-related illness. The majority of heat-related deaths occur in urban areas, where stagnant air and poor ventilation are common.11 Between 35% and 45% of the elderly live in urban areas, where they tend to reside in older apartment buildings in which air conditioning is not readily available.12 Many exist on a very limited income and may be unableto afford sufficient air conditioning. Additionally, many elderly individuals live alone and have little outside social contact, effectively isolating them and preventing access to a cooler environment during a heat wave.13,14
Heat illness is rarely reported among the retired populations living in high-heat climates, such as the desert, largely because in these environments air conditioning is readily available. This illustrates perhaps the most important factor in prevention of heat-related illness—access to air conditioning. Older people who have access to an airconditioned place, even just the lobby of their apartment building, are less likely to suffer a heatrelated illness.12 The increased use of air conditioners has been postulated to be a significant factor in the decrease in heat-related deaths in both the United States and England.15 Shopping malls, public libraries, and heat wave shelters are air-conditioned environments that the elderly should be encouraged to take advantage of, even if for only part of the day.16
Prevention messages that encourage older individuals to spend time in cool environments provided via radio and television media should be disseminated to the public as early as possible when high temperatures/humidity are predicted. Direct advice from healthcare providers (see the Patient Tearout, “When It Gets Hot Outside”), as well as visiting home health aides, Meals-on-Wheels personnel, postal service workers, neighbors, and family members, are also important to encourage vulnerable older individuals to take advantage of air-conditioned environments during heat waves. Some cities have developed networks of police officers, social workers, and volunteers to keep tabs on their most vulnerable citizens during times of extreme temperature. For example, Chicago has an automated phone system that calls some 60,000 seniors and frail or disabled persons living in the community. When there is no answer, a team is sent to make a personal visit to check on the individual.
MINOR HEAT-RELATED ILLNESSES
Heat Cramps
Heat cramps are brief, intermittent, and often severe muscular cramps in muscles that are fatigued, usually in individuals who have produced copious amounts of sweat with hypotonic fluid replacement during exertion. The cramps are often associated with exertion in a hot environment, but with increased age may occur in individuals in more temperate climates. Pathophysiologically, heat cramps appear to be related to salt deficiency, as victims exhibit hyponatremia, hypochloremia, and low urinary sodium and chloride levels. Essentials of diagnosis include cramps of the most-worked muscles after a period of exertion.
As a general rule for all heat-related illness, the individual should be removed from the hot environment, and exertion should be avoided. Treatment of heat cramps consists of oral fluid and salt replacement with a 0.1% to 0.2% water/salt solution. Severe cases require intravenous normal saline solutions (0.9% NaCl).4 Heat cramps usually disappear rapidly after treatment begins, and there are no significant lasting effects.
Heat Edema
Heat edema manifests as swollen feet and ankles, and is reported by individuals—typically the elderly— who encounter climatic stresses of tropical and subtropical areas. The swelling is minimal, with little or no functional impairment, and generally selfresolves after several days.17 The exact pathophysiology is unknown, but venostasis with orthostatic pooling from prolonged sitting or standing, leading to accumulation of interstitial fluid in the lower extremities, is believed to be the likely mechanism. Treatment consists of simple leg elevation or support hose. Symptoms remit spontaneously or when the individual leaves the hot area.
Heat Syncope
Heat syncope is another heat illness with a predilection toward the elderly and may be precipitated by dehydration.18 The individual experiences a prolonged period of dizziness, sometimes with an acute loss of consciousness. This may result in a fall, which among the elderly may result in serious injury. It is believed that peripheral vasodilatation, necessary for heat dissipation, causes a reduction in the thoracic blood volume. This peripheral pooling, when combined with a prolonged period of standing or a rapid transition from sitting to standing, may inhibit adequate cerebral perfusion to maintain consciousness.
Treatment consists of avoidance of prolonged standing, oral volume replacement, and lying recumbent. The patient should be instructed to move often and flex leg muscles when standing stationary. Elderly patients who have a heat syncopal episode are much more likely to have another in the future, and should be educated to recognize the warning signs, such as scotomata, tunnel vision, vertigo, nausea, diaphoresis, and weakness. Upon recognition of these symptoms, the individual should assume a sitting or horizontal position until the condition resolves.
Prickly Heat
This condition is also known as miliaria rubra, lichen tropicus, and, most commonly, “heat rash.” It is an acute inflammatory disorder of the skin that occurs in hot and humid climates. The rash is the result of blockage of sweat gland pores by macerated epidermal layers. Clinically, the rash appears as pruritic vesicles on an erythematous base. The rash is usually limited to areas covered by clothes, especially the upper arms and legs. The area with the rash is usually anhydrotic, and if left untreated a chronic dermatitis may develop. The elderly are particularly susceptible because of agerelated skin changes and decreased heat perception that leads to the wearing of constrictive and overly warm clothing.
Treatment consists of using a chlorhexidine cream or lotion. Salicylic acid 1% may also by used (3 times daily) but with extreme caution in the older individual because salicylate intoxication can occur.4 Wearing light, loose-fitting clothing and using air conditioning is an effective prevention strategy.
HEAT EXHAUSTION
Heat exhaustion is the most common form of heat-related illness encountered by healthcare providers. It is a more serious heat-related entity that falls between minor heat illnesses and critical heat stroke. This condition is seen in both the young who are exerting themselves and in the sedentary elderly. Heat exhaustion is a clinical syndrome characterized by volume depletion under conditions of heat stress that can be divided into two types: water depletion and salt depletion.15 Water depletion heat exhaustion is due to inadequate hydration. Older individuals who are invalid and who do not have free access to water are most susceptible to this form. If fluid volumes are not restored, water depletion heat exhaustion will progress into heat stroke.19 Salt depletion heat exhaustion takes longer to develop, and occurs when large volumes of thermal sweat are replaced by solutions containing inadequate sodium. Identifying pure types of either form of depletion are rare, as most cases of heat exhaustion involve both water and salt depletion.
The symptoms of heat exhaustion are variable and nonspecific, and include profuse sweating, malaise, headache, dizziness, anorexia, nausea, vomiting, vertigo, chills, muscle or general weakness, tachycardia and hypotension, visual disturbances, and cutaneous flushing. Core temperature is often normal but may be elevated. If a rise in core temperature is recorded, it should be less than 40 degrees C (104 degrees F). Mental function should be intact with no CNS dysfunction. Any CNS disturbances (eg, seizures, coma) with elevated core temperatures suggest that the condition has progressed to heat stroke.20,21
Treatment must be individualized on the basis of the exam and laboratory findings. Rest in a cool environment with avoidance of heat stress is universal and should begin immediately. Decisions regarding the type of fluid and electrolyte replacements should be assessed clinically via blood pressure, pulse, and orthostatic changes. Oral hydration is allowed in patients who are cognitive and have no gastrointestinal symptoms, but may provoke vomiting in some cases.
Recovery should be rapid once treatment has been initiated, usually within 2-3 hours. Older patients, particularly those with cardiovascular disease or other predisposing factors, require more cautious fluid and electrolyte replacement and frequent reassessment. Elderly individuals suffering heat exhaustion are therefore best managed in a hospital. Treatment must be patient-specific, as failures to accurately treat heat exhaustion may lead to heat stroke.
HEAT STROKE
Heat stroke is the rarest and the most serious of all heat-related illnesses. It is a true medical emergency with high rates of associated morbidity and mortality, particularly among the older population. In heat stroke, there is impairment of the thermoregulatory mechanisms. While these mechanisms remain intact in the previously discussed conditions, in heat stroke they fail, allowing core body temperature to rise to at least 40.5 degrees C (104.5 degrees F), and often higher than 41 degrees C (106 degrees F).22 This uncontrolled rise in core temperature produces multisystem tissue damage and organ dysfunction.
Heat stroke is divided into two categories. The first, exertional or sporadic heat stroke, is usually found in young individuals involved in extreme physical activity. The second type, classical or epidemic, is more commonly found in the elderly, especially those who are chronically ill and sedentary.23 Classical heat stroke can develop slowly over several days, presents with minimally elevated core body temperature, little sweating, and minimal laboratory abnormalities, which contribute to its underrecognition. It occurs during periods of sustained high temperatures, and disproportionately affects the elderly due to risk factors discussed above, including multiple chronic diseases, medication use, social isolation, and residence in poorly ventilated homes without air conditioning. On the other hand, in exertional heat stroke, sweating is usually present and there are often markedly abnormal laboratory findings, such as lactic acidosis, severe rhabdomyolysis, hypocalcemia, hypoglycemia, and acute renal failure. The underlying mechanism in classical heat stroke is poor dissipation of environmental heat in contrast to exertional heat stroke, where there is endogenous heat production.5
Symptoms of heat stroke include hyperpyrexia with exposure to heat stress. Core body temperature will usually be at least 41 degrees C (106 degrees F) but may be higher. All temperatures should be measured with a rectal, esophageal, or bladder probe. Signs of severe central nervous dysfunction (coma, seizures, delirium) are usually present. Anhydrosis is common in the patient experiencing classical heat stroke; however, the presence of sweat is not unusual. Other signs include tachycardia, tachypnea, and hypotension. A complete medical work-up must be done, including chest x-ray, electrocardiogram, arterial blood gas analysis, complete blood count, liver function tests, and urinalysis to evaluate for other causes of hyperpyrexia.
Treatment of heat stroke must be initiated immediately and aggressively, as the more prolonged the episode, the worse the predicted outcome. Rapid cooling is essential, and the core temperature should be brought down to 38.8 degrees C (101.8 degrees F). Cooling modalities include ice water immersion or evaporative cooling using large circulating fans and skin wetting. Intravenous fluids should be given modestly due to considerable organ and system damage associated with heat stroke. For many elderly patients, these systems have been previously compromised from chronic medical conditions. This necessitates that medical management shift to treating these complications once the initial heat crisis has been controlled.
CONCLUSION
Heat-related illness disproportionately affects the elderly. Deaths from heat-related illness among the elderly are small compared to other ailments that lead to mortality among the older population. However, heat-related illness, with all of its associated morbidity and mortality, is totally preventable. Simple public health initiatives during times of sustained increased climatic temperature that identify the elderly at risk and then target these individuals with the necessary aid are effective means of addressing the problem. Preventable measures have often been too little too late, and the response of healthcare providers delayed. Education of healthcare providers and the elderly is paramount to avoid unnecessary illness and death with the next heat wave, wherever that strikes.
The cure for heat-related illness does not require extensive research, testing, or funding. Communities already have the resources and knowledge to prevent the problem. It’s a matter of increased awareness by healthcare providers and coordination of services to ensure they reach those most at risk who need them.
1. Becerra H, Covarrubias A. Elderly, isolated are heat’s quiet victims. Los Angeles Times. July 29, 2006:A.1.
2. Wongsurawat N, Davis BB, Morley JE. Thermoregulatory failure in the elderly. St. Louis University Geriatric Rounds. J Am Geriatr Soc 1990;38:899-902.
3. Nakayama T, Eisenman JS, Hardy JD. Single unit activity of anterior hypothalmus during local heating. Science 1961;134:560-561.
4. Simon E. Paradigms and concepts in thermal regulation of homeotherms. News Physiol Sci 1987;2:89-95.
5. Khosla R, Guntupalli KK. Heat-related illnesses. Crit Care Clin 1999;15(2):251-263.
6. Kilbourne EM, Choi K, Jones S, Thacker SB. Risk factors for heatstroke. A case study. JAMA 1982;247:3332-3336.
7. Heat-related mortality–United States, 1997. MMWR Morb Mortal Wkly Rep 1998;47:473-476.
8. Kuczmarski R, Flegal K, Campbell S, Johnson CL. Increasing prevalence of overweight among US adults. The National Health and Nutrition Examination Surveys (NHANES), 1960 to 1991. JAMA 1994;272(3):205-211.
9. Families USA. Cost overdose: Growth in drug spending for the elderly, 1992-2010. Washington: Families USA. Available at: www.familiesusa.org. Accessed April 19, 2007.
10. Hanlon JT, Fillenbaum GG, Ruby DM, et al. Epidemiology of over-the-counter drug use in community dwelling elderly: United States perspective. Drugs Aging 2001;18(2):123-131.
11. Shen T, Howe H, Alo C, Moolenaar RL. Toward a broader definition of heat-related death: Comparison of mortality estimates from medical examiners’ classification with those from total death differentials during the July 1995 heat wave in Chicago, Illinois. Am J Foresnsic Med Pathol 1998;19(2):113-118.
12. Centers for Disease Control and Prevention. Heat-related illnesses and deaths–Missouri, 1998, and United States, 1979-1996. JAMA 1999;282(3):227-228.
13. Semenza JC, Rubin CH, Falter KH, et al. Heat-related death during the July 1995 heat wave in Chicago. N Engl J Med 1996;335:84-90.
14. Naughton MP, Henderson A, Mirabelli MC, et al. Heatrelated mortality during a 1999 heat wave in Chicago. Am J Prev Med 2002;22(4):221-227.
15. Donaldson GC, Keatinge WR, Nayha S. Changes in summer temperature and heat-related mortality since 1971 in North Carolina, South Finland and Southeast England. Environ Res 2003;91:1-7.
16. From the Centers for Disease Control and Prevention. Heatrelated deaths–Dallas, Wichita, and Cook Counties, Texas, and United States, 1996. JAMA 1997;278(6):462-463.
17. Tek D, Olshaker J. Heat-illness. Emerg Med Clin North Am 1992;10(2):299-310.
18. Sterner S. Summer heat illnesses. Conditions that range from mild to fatal. Postgrad Med 1990;87(8):67-70, 73.
19. Hubbard RW, Gaffin, Squire DL. Heat related illness. In: Auerbach PS, ed. Wilderness Medicine: Management of Wilderness and Environment Emergencies. 3rd ed. St. Louis, MO: Mosby; 1995:167-212.
20. Lee-Chiong TL Jr, Stitt J. Heatstroke and other heat-related illnesses. The maladies of summer. Postgrad Med 1995;98(1):26-28, 31-33, 36.
21. Waters TA. Heat illness: Tips for recognition and treatment. Cleve Clin J Med 2001;68(8):685-687.
22. Barrow M, Clark KA. Heat-related illnesses. Am Fam Physician 1998;58(3):749-756.
23. Weisskopf MG, Anderson HA, Folds S, et al. Heat wave morbidity and mortality, Milwaukee, Wis, 1999 vs 1995: An improved response? Am J Public Health 2002;92(5):830-833.