
Peer Reviewed
Actinomycotic Osteomyelitis of the Left Lower Jaw
AUTHOR:
Nishit Harishbhai Patel, MD
Assistant Professor, Department of Pediatrics, Division of Pediatric Emergency Medicine, UT Southwestern Medical Center, Dallas, Texas
Citation: Patel NH. Actinomycotic osteomyelitis of the left lower jaw [published online November 26, 2018]. Infectious Diseases Consultant.
A 17-year-old male adolescent presented to our emergency department (ED) with a 1-week history of left lower jaw pain and swelling. He also had had a fever, with a temperature as high as 38.9°C, and poor oral intake for 24 hours prior to presentation.
History. The patient recently had been given a course of amoxicillin by his dentist for left-side lower third molar dental disease while waiting to see an oral surgeon for extraction. He had taken the antibiotic for 5 days, but the pain and swelling had worsened, prompting him to come to the ED.
Two years prior to presentation, he had experienced a toothache and left lower jaw swelling, which had resolved with over-the-counter pain medications without his having sought any medical care. Later, 2 to 3 months prior to this ED visit, he had had a similar episode of left-sided lower jaw swelling with toothache, which had resolved after a 10-day course of oral antibiotics along with pain medications.
His surgical history included a left patellar tendon repair 4 years ago. His family history was unremarkable. His immunizations were up to date.
Physical examination. His vital signs at presentation included a temperature of 38°C, heart rate of 98 beats/min, respiratory rate of 18 breaths/min, blood pressure of 120/74 mm Hg, and oxygen saturation of 99% on room air. He was awake and alert but in severe pain.
Oral examination findings included some degree of trismus. A dental cavity was visible on the left lower third molar, with surrounding gingival swelling and tenderness. There was no active pus drainage. An ill-defined indurated swelling measuring approximately 8 x 5 cm was present on his left lower jaw, extending to the submandibular region, which was firm, warm, and tender to the touch. The rest of the physical examination findings were unremarkable.
Diagnostic tests. Result of a complete blood cell count and a comprehensive metabolic panel were unremarkable except for an elevated white blood cell (WBC) count of 17,500/µL with a left shift (83% neutrophils). His C-reactive protein (CRP) level of 187 mg/dL (reference range, 0-10 mg/dL) and his erythrocyte sedimentation rate (ESR) of 95 mm/h (reference range, 0-20 mm/h) were elevated.
A computed tomography (CT) scan of the facial bones with contrast (Figures 1 and 2) showed left mandibular osteomyelitis and an adjacent large tooth abscess measuring up to 5 cm.
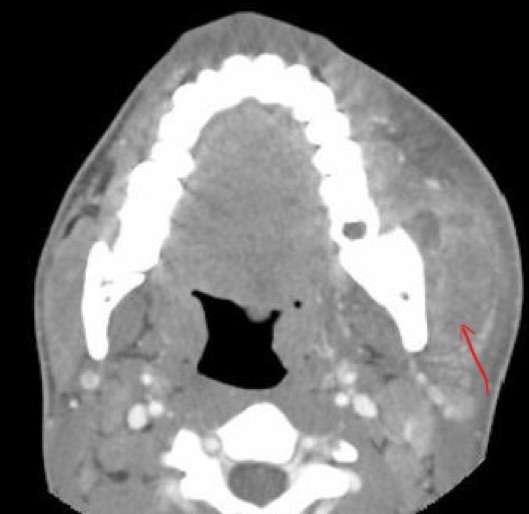
Figure 1. Axial contrast-enhanced CT image showing an abscess (complex multilocular fluid collection) in the left masticator space, primarily lateral and inferior to the mandibular angle (red arrow).
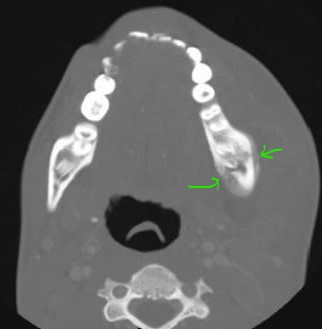
Figure 2. Changes of osteomyelitis (bony destruction with new periosteal reaction) secondary to dental disease (green arrow) were seen on bone window settings.
The patient was started on intravenous antibiotics (ceftriaxone and clindamycin). He underwent for incision and drainage for the tooth abscess, with extraction of the left molar, debridement, and bone biopsy. Blood cultures did not grow any organism. His tissue fungal and acid-fast bacilli cultures were negative. Tissue aerobic culture grew polymicrobial organisms (Streptococcus anginosus, Eikenella corrodens, and Streptococcus oralis/Streptococcus mitis), and anaerobic culture grew Prevotella oralis, Prevotella melaninogenica, and Bifidobacterium species. Pathology test results of the specimens showed changes consistent with chronic osteomyelitis, positive silver methenamine stain, and bacteria that were morphologically consistent with Actinomyces species, with absence of malignant cells.
Treatment. The patient received intravenous antibiotics for 7 days during his hospitalization. His condition improved clinically, and laboratory test results at discharge had improved, with a WBC count of 12,300/µL, a CRP level of 21 mg/dL, and an ESR of 20 mm/h. The infectious disease team was consulted during hospitalization, and the patient was sent home on a 12-month course of oral amoxicillin to treat actinomycotic osteomyelitis.
Outcome of the case. The patient was seen for follow-up in the infectious disease clinic at 3, 6, and 12 months, with complete resolution of symptoms and without any recurrence of disease.
Discussion. Pediatric actinomycosis is an indolent, uncommon, and invasive suppurative infection, most commonly affecting the cervicofacial region (approximately 50% of cases), but many other sites of infection have been described in the literature. It is caused by an anaerobic or microaerophilic, non–acid-fast, gram-positive bacteria, primarily from the genus Actinomyces, which normally colonize the oral cavity, gastrointestinal tract, and genital tract. The source of human infection is almost always endogenous flora.1-5 Patients with cervicofacial actinomycosis often have a history of poor dental hygiene, oral trauma, and/or oral surgery that facilitates entry of organisms into cervicofacial tissues.4-6
Cervicofacial actinomycosis usually manifests as a painless, slow-growing, hard mass and can produce cutaneous a sinus tract or fistula, a condition commonly known as lumpy jaw. Less frequently, it manifests clinically as an acute pyogenic infection with a tender, fluctuant mass with trismus. Bone is not involved early in the disease process.1
Actinomycotic osteomyelitis is an unusual clinical entity in the pediatric population. The mandible is the most commonly reported site of infections among pediatric cases. Most reported cases of mandibular osteomyelitis attributable to Actinomyces became chronic.7 This may be because the clinical manifestations are often subtle, and the diagnosis is typically delayed for weeks to months.
Imaging studies (CT or magnetic resonance imaging), examination of bacterial cultures, and cytopathologic assessment of tissues and secretions collected at the infection site are very useful in diagnosis. Given that actinomycosis is usually polymicrobial, other organisms are almost always cultured from biopsies performed for mandibular osteomyelitis,2,7,8 as was reported in our patient’s case.
Medical and surgical intervention is very important in the management of actinomycosis. Penicillin G is usually the drug of choice regardless of the severity and site of actinomycosis. Actinomyces species are usually susceptible to penicillin, ampicillin, clindamycin, and tetracycline/doxycycline, all of which should penetrate well into bone. The duration of treatment depends on the site and extent of infection. Most experts recommended 3 to 12 month of therapy, including intravenous and oral therapy.1,8-11
Surgical intervention includes incision and drainage for abscesses and debridement of infected tissue. Adequate debridement is the cornerstone of therapy, with all actinomycotic osteomyelitis cases reported in the literature eventually requiring at least 1 debridement.7
Cervicofacial actinomycosis poses a diagnostic challenge. A high index of suspicion is required, and it should be in the differential diagnosis of any soft-tissue swelling of the head and neck in the pediatric population.
References:
- Sharkawy AA. Cervicofacial actinomycosis and mandibular osteomyelitis. Infect Dis Clin North Am. 2007;21(2):543-556.
- Pulverer G, Schütt-Gerowitt H, Schaal KP. Human cervicofacial actinomycoses: microbiological data for 1997 cases. Clin Infect Dis. 2003;37(4):490-497.
- Bennhoff DF. Actinomycosis: diagnostic and therapeutic considerations and a review of 32 cases. Laryngoscope. 1984;94(9):1198-1217.
- Smego RA Jr, Foglia G. Actinomycosis. Clin Infect Dis. 1998;26(6):1255-1261.
- Brown JR. Human actinomycosis: a study of 181 subjects. Hum Pathol. 1973;4(3):319-330.
- Feder HM Jr. Actinomycosis manifesting as an acute painless lump of the jaw. Pediatrics. 1990;85(5):858-864.
- Robinson JL, Vaudry WL, Dobrovolsky W. Actinomycosis presenting as osteomyelitis in the pediatric population. Pediatr Infect Dis J. 2005;24(4):365-369.
- Heo SH, Shin SS, Kim JW, et al. Imaging of actinomycosis in various organs: a comprehensive review. Radiographics. 2014;34(1):19-33.
- Thacker SA, Healy CM. Pediatric cervicofacial actinomycosis: an unusual cause of head and neck masses. J Pediatric Infect Dis Soc. 2014;3(2):e15-e1
- Brook I. Actinomycosis: diagnosis and management. South Med J. 2008;101(10):1019-1023.
- LeCorn DW, Vertucci FJ, Rojas MF, Progulske-Fox A, Bélanger M. In vitro activity of amoxicillin, clindamycin, doxycycline, metronidazole, and moxifloxacin against oral Actinomyces. J Endod. 2007;33(5):557-560.