
Peer Reviewed
Palmar Lesions in a Sexually Active Man
Authors:
John F. Linabury, DO
Diving Medical Officer, US Navy Department of Medicine, Falls Church, Virginia
Andrew M. Basnett, MD
Dermatologist, Naval Health Clinic Makalapa, Joint Base Pearl Harbor-Hickam, Hawaii
Citation:
Linabury JF, Basnett AM. Palmar lesions in a sexually active man [published online December 11, 2018]. Infectious Diseases Consultant.
Disclaimer:
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, the Department of Defense, or the US Government. John Linabury and Andrew Basnett are military service members. This work was prepared as part of their official duties. Title 17 USC § 105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 USC § 101 defines a US Government work as a work prepared by a military service member or employee of the US Government as part of that person’s official duties.
A 24 year-old man presented to the dermatology clinic with a 3-month history of a pruritic, scaly, papular eruption across his upper and lower extremities, abdomen, neck, and genital areas, as well as hyperpigmented palmar macules.
History. The patient previously had received a diagnosis of prurigo nodularis from his primary care physician, for which he had been treated unsuccessfully with a topical high-potency corticosteroid. His medical history was significant for a remote history of a sexually transmitted infection and unprotected intercourse with 1 partner over the past year. He denied any previous anogenital ulceration, oral lesions, or hair loss, and findings of a review of systems were noncontributory.
Physical examination. Skin examination revealed multiple thick, scattered, scaly papules with occasional collarets ranging in size from 4 mm to 1.5 cm across the upper and lower extremities (Figure 1), abdomen (Figure 2), neck, and genitals. Hyperpigmented circular macules were present on palmar surfaces bilaterally (Figure 3). Inguinal, axillary, and cervical lymphadenopathy was present.

Figure 1.

Figure 2.
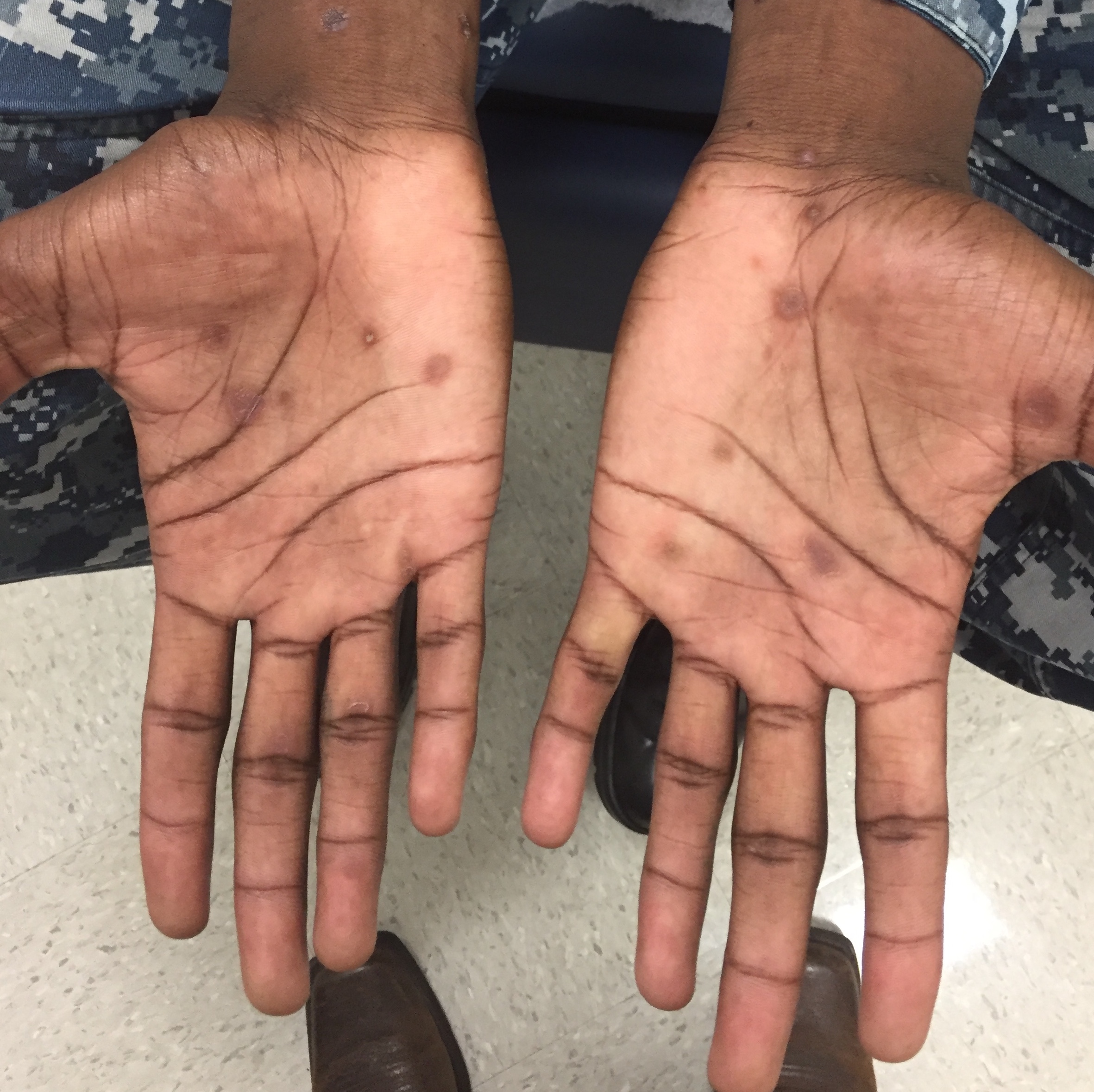
Figure 3.
Diagnostic tests. Results of rapid plasma reagin (RPR) were reactive at a 1:128 dilution. Results of a previous RPR performed 6 weeks prior had been equivocal, with repeat testing recommended. Treponema pallidum antibody test results were positive. Results of HIV 1 and 2 antibody tests, a gonococcal/chlamydial urine DNA probe, and a hepatitis panel were negative. Urinalysis and urine culture results were normal.
Punch biopsy of the lesions was performed, the results of which showed superficial perivascular dermatitis with plasma cells, lymphocytes, and histiocytes. Treponemal immunohistochemical stain was positive for numerous organisms. The histology test findings were consistent with secondary syphilis.
Discussion. The patient’s clinical history was highly suspicious for secondary syphilis, with the results of further testing ultimately being confirmatory. Syphilis is known for having variable clinical and histopathologic findings, imparting the necessity for a high degree of clinical suspicion.
The historic nadir for the US incidence of primary and secondary syphilis was 2000; since then, the primary and secondary syphilis incidence rates increased each year as reported through 2016. During 2016, national syphilis rates increased 17.6% compared with 2015, the highest rate reported since 1993.1 The Centers for Disease Control and Prevention reported an increased incidence from 2015 to 2016 regardless of sex, sexual behavior, region, ages, and ethnicity. The highest incidences were found among men who have sex with men, men aged 20 to 24 years, and black men. All US regions had an increased reported incidence rate during 2016, with the West having the highest rate of reported cases (11.4 cases per 100,000 population).1 An increased rate of syphilis among women since 2012 has been accompanied by an increase in congenital syphilis cases, increasing both maternal and fetal morbidity and mortality.1 Syphilis infection raises the likelihood of HIV infection, and coinfection with HIV modifies the presentation, efficacy of treatment, and disease monitoring of syphilis.
Syphilis has protean cutaneous manifestations and to this day retains the moniker “the great imitator.”2,3 That syphilis often is divided into imprecise stages of presentation and durations compounds this truth. Primary syphilis is often a painless anogenital chancre (ulcer) without lymphadenopathy or constitutional symptoms. Secondary syphilis often demonstrates a typical papulosquamous eruption on the trunk and acral surfaces accompanied by constitutional symptoms (eg, malaise, headache, nausea, anorexia, arthralgias, bone pain) and signs (eg, fever, conjunctivitis, uveitis, hepatosplenomegaly, elevated liver enzymes, jaundice, and lymphadenopathy). Less frequently, an atypical presentation, syphilitic alopecia, or condylomata lata are evident. The spectrum of typical and atypical presentations increases with HIV coinfection.3
Papulosquamous palmar and plantar lesions should immediately raise concern for syphilis and several other etiologies, regardless of the patient’s immune status. Latent syphilis, both early and late, demonstrates serologic evidence with a paucity or absence of mucocutaneous findings. Following a period of latency, tertiary syphilis may develop and present with gummatous, cardiovascular, or central nervous system inflammation. It is germane to note that neurosyphilis can occur across this spectrum of presentations and time course.2,3
The diagnosis hinges on clinically relevant information combined with nontreponemal and treponemal serologic tests. The primary screening nontreponemal tests are RPR and the VDRL test, which can provide quantitative information with serial dilutions. If results are positive, this test is followed with more-specific treponemal tests such as the fluorescent treponemal antibody absorption (FTA-ABS) test, microhemagglutination assay for T pallidum (MHA-TP), or hemagglutination treponemal test for syphilis (HATTS). These serologic tests have a risk of false-positive results.
Darkfield microscopy remains the gold standard, but it is technically demanding. Biopsy of questionable lesions can help refine the diagnosis. Under light microscopy, hematoxylin and eosin staining can demonstrate endothelial edema, edema to the superficial and deep perivascular epidermal and dermal spaces, plasma cell–predominant infiltrate, lymphocyte and histiocyte infiltrates, epidermal dermal junction changes, epidermal hyperplasia, or mixed patterns.4,5 Silver staining, while not specific for spirochetes, and immunohistochemical staining can be employed for equivocal cases.4
Treatment reduces symptoms, transmission, and the likelihood of complications. Parenterally administered benzathine penicillin G, 2.4 million units, remains the treatment of choice in all stages of syphilis. The duration and frequency change based on the patient’s immune status or suspicion of neurosyphilis. Persons with a penicillin allergy are recommended to undergo desensitization. The Jarisch-Herxheimer reaction, an immune response due to lysing of spirochetes, can present in the first 24 hours of treatment.
Monitoring treatment over a 6- to 12-month period, evaluating for a 4-fold decline in RPR results is considered successful (1:128 to 1:32 in our patient’s case). The nontreponemal tests demonstrate a more rapid decline with successful treatment, whereas treponemal test results frequently remain elevated over this same 12-month period. HIV coinfection produces variable outcomes during the monitoring process. Persons suspected of having primary or secondary syphilis should be tested for HIV.
In our patient’s case, initial RPR test results were equivocal, and the patient did not recall any history of genital ulcers. In previous cases presented to our clinic, nonspecific symptoms associated with secondary syphilis are the first presentation encountered by primary care providers, often leading to delay in diagnosis. Due to syphilis’s varied clinical presentation and the concerning upward trajectory of incidence rates in all regions of the country, clinicians should maintain a high degree of suspicion with a low threshold for further testing.
- 2016 sexually transmitted diseases surveillance. Centers for Disease Control and Prevention. https://www.cdc.gov/std/stats16/default.htm. Accessed November 20, 2018.
- Balagula Y, Mattei PL, Wisco OJ, Erdag G, Chien AL. The great imitator revisited: the spectrum of atypical cutaneous manifestations of secondary syphilis. Int J Dermatol. 2014;53(12):1434-1441.
- Hook EW III, Marra CM. Acquired syphilis in adults. N Engl J Med. 1992;326(16):1060-1069.
- Hoang MP, High WA, Molberg KH. Secondary syphilis: a histologic and immunohistochemical evaluation. J Cutan Pathol. 2004;31(9):595-599.
- Jeerapaet P, Ackerman AB. Histologic patterns of secondary syphilis. Arch Dermatol. 1973;107(3):373-377.