
Peer Reviewed
Hidradenitis Suppurativa
Author:
Joe R. Monroe, MPAS, PA
Epiphany Dermatology, Tulsa, Oklahoma
Citation:
Monroe JR. Hidradenitis suppurativa [published online February 11, 2019]. Consultant360.
A 39-year-old woman self-referred to a dermatology practice for evaluation of a skin condition that had been present since puberty, waxing and waning, often paralleling her menstrual cycle.
According to the patient, the condition involved the frequent appearance of “boils,” painful lumps, and constant irritation in the affected areas. She was also distressed about having so many “blackheads” in her axillae and on her chest.
A similar condition had affected other family members, all women, all beginning at puberty.
This patient had been treated with topical retinoids, topical antibiotics, and oral antibiotics, to no good effect.
The patient reported a 15-year history of smoking.
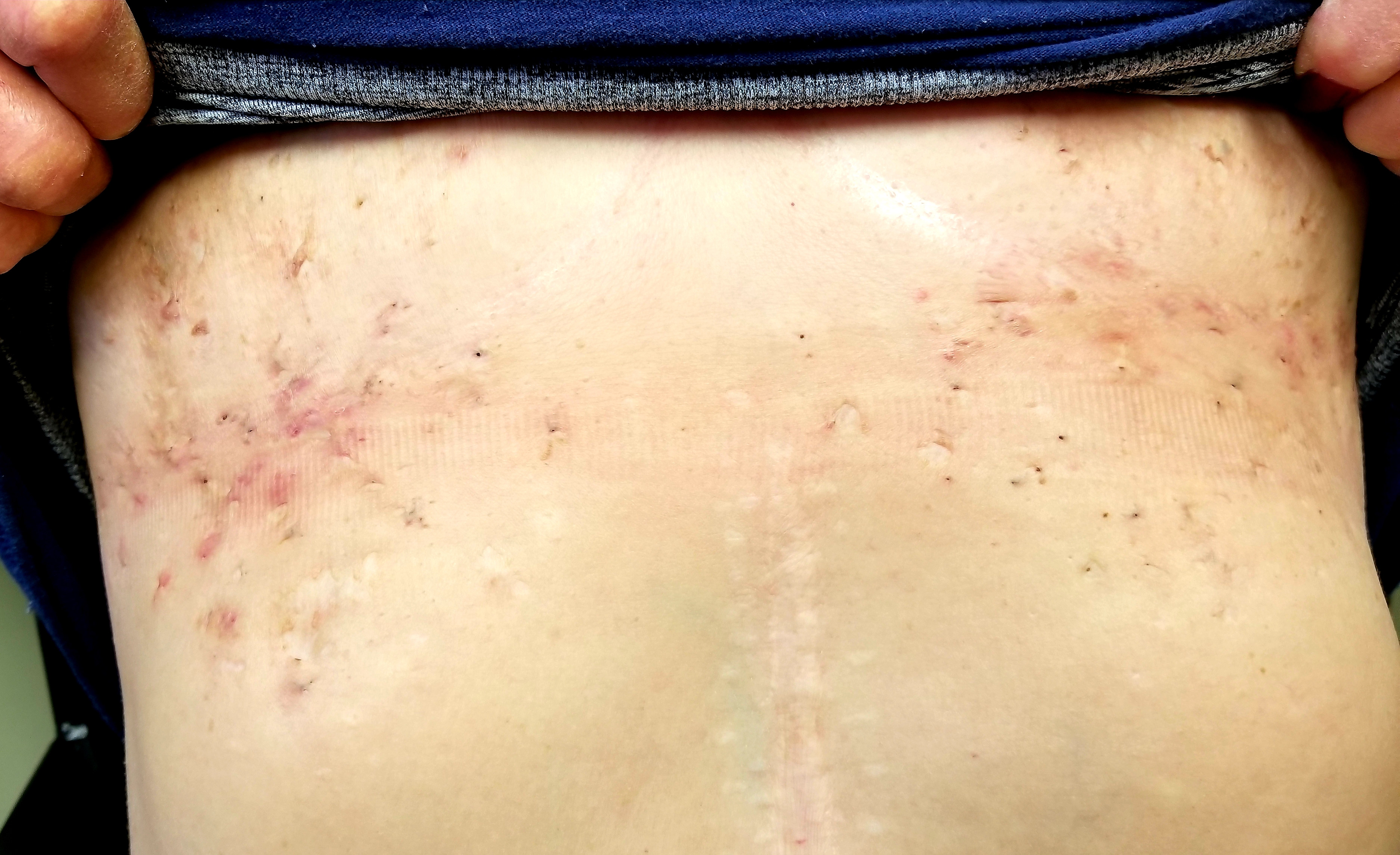
Physical examination. The patient’s chest and axillae were covered with dense collections of open comedones, red inflamed papules, and a few inflamed tender nodules (Figures). There was minimal scarring. Her groin and intergluteal areas were free of any such lesions. The patient was quite obese, weighing almost twice as much as normal for her height.

Discussion. This patient has a relatively mild case of hidradenitis suppurativa (HS), which was first described by French surgeon Alfred Velpeau in the 1830s. Since then, the condition has been named and renamed, with terms such as acne inversus and Verneuil disease. In more modern times, it has become generally accepted that HS represents a disease of the apocrine glands, or possibly of dysfunctional pilosebaceous units, inside of which sweat and oil are trapped, setting off an inflammatory response that clearly differs from acne vulgaris.
This patient’s case is relatively mild, but many are not as fortunate, often suffering from large, painful, fluid- and pus-filled cysts that frequently connect by way of subcutaneous tracts. They are confined to areas rich in apocrine glands and appear to be related to a number of factors such as heredity (in approximately one-third of cases), obesity, and smoking, the latter two as exacerbating but not causative factors.
Most HS cases begin with the onset of puberty, strongly suggesting a role for hormones.
HS is considered to be part of what Plewig and Kligman called the “acne tetrad,” which includes HS, acne conglobata, dissecting cellulitis of the scalp, and pilonidal sinus. This author has failed to see this combination in more than 35 years practicing dermatology. Likewise, the literature relates that two-thirds of HS cases occur in women, but in this author’s experience, the ratio is more like 20 to 1, female to male.
HS is far from rare, affecting between 1% and 4% of the population, and yet it is often misdiagnosed and treated as “boils” or methicillin-resistant Staphylococcus aureus infection. The keys to diagnosis are the onset at puberty; the presence of numerous open comedones, inflamed cysts, and, in advanced cases, extensive ropy scarring; and involvement of apocrine gland–rich intertriginous areas.
The differential diagnosis does include abscesses or carbuncles, but bacterial cultures of HS lesions yield only normal mixed flora.
A staging system has been developed for HS, called the Hurley scale, which uses 3 classes: class I, no sinuses or scarring but may have solitary or multiple lesions; class II, recurrent lesions with sinus tract formation (one or more) and widely scattered scarring; and class III, diffuse distribution of lesions with multiple sinus tracts and scars, with no intervening normal skin. Our patient’s mild case is illustrative of class I.
Although HS in well known among dermatologists, it is often unknown and therefore misdiagnosed in other specialties. Incision and drainage procedures are not especially helpful, nor are oral antibiotics, since HS is not an infection.
Surgical removal of the affected tissue in large swaths effectively removes most of the apocrine glands in the treated area. Obviously, this option involves the need for a general surgeon, general anesthesia, and the usual risks attendant with any large surgical procedure. Isolated painful lesions can be incised and drained for relief, although this is approach is not indicated for multiple sites. One of the more effective nonsurgical options has been the approval for the use of adalimumab, a tumor necrosis factor α inhibitor, but this is relatively expensive and requires initial and ongoing bloodwork along with patient-administered injections. Although theoretically possible, serious potential adverse effects associated with the use of adalimumab as monotherapy have proven to be quite rare.