
Peer Reviewed
Extreme Hypercalcemia of Malignancy
Authors:
Ryan Rohan Sanni
Windsor University School of Medicine, Cayon, Saint Kitts and Nevis
Krishdeep Khosla, MD
Mt. Sinai Health System Chicago, Illinois
Venugopala Bheemanathini, MD
RMC Stringfellow Memorial Hospital, Anniston, Alabama
Dyan Cristyn Alvarez Dupaya, MD
Jackson Park Hospital, Chicago, Illinois
Citation:
Sanni RR, Khosla K, Bheemanathini V, Dupaya DCA. Extreme hypercalcemia of malignancy [published online February 15, 2019]. Consultant360.
A 70-year-old woman presented to an outpatient clinic with constant, unremitting sharp pain in the left lateral lumbar spine, which she rated as 8 of 10 in severity. The pain had been present for the past 48 hours and had progressively become more severe within 24 hours, with radiation to the mid thoracic spine. She also reported having severe constipation for the past 4 days despite the use of laxatives, and loss of appetite throughout the day for the past 14 days.
Early the next morning, the patient was admitted to the hospital with severe nausea and vomiting associated with increasing pain in the lumbar spine, now rated as 9 of 10. Results of laboratory tests done in the emergency department (ED) were significant for a total serum calcium level of 17.8 mg/dL (reference range, 8.4-10.2 mg/dL). Very few cases of hypercalcemia bordering 18 mg/dL or above have been reported worldwide, making this case unique from other cases of similar presentations.
On further history-taking in the ED, the patient reported having had a lump in the right breast accompanied by nipple discharge for the past 3 weeks. During physical examination of the right breast, dense breast tissue was felt in the right lateral quadrant with an accompanying mass measuring approximately 3 cm. Mammography of the right breast was done in the hospital, and the results showed an area of architectural distortion with associated calcifications, and a suspicious lymph node with associated calcifications, findings that were highly suggestive of malignancy with a likelihood of 95% or greater (Figure 1).
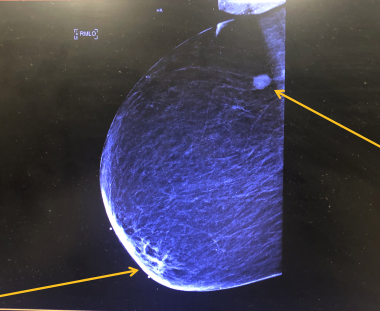
Figure 1. The arrow on the bottom left represents an area of architectural distortion with associated calcifications, and the arrow in the upper right represents a suspicious lymph node with associated calcifications. Both of these findings were highly suggestive of malignancy with a likelihood of 95% or greater as per the radiology and pathology departments.
Given the suspicious mammography findings, ultrasound-guided core needle biopsy of the right breast was performed. The results demonstrated a pathologic lymph node with calcifications, corresponding with the mammography findings (Figure 2).
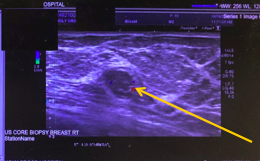
Figure 2. Ultrasound-guided core needle biopsy of the right breast demonstrated a pathologic lymph node (arrow) with calcifications corresponding with the mammography findings. The lymph node was confirmed to be malignant by the pathology department after biopsy.
Histopathological biopsy results of the lymph node confirmed the presence of metastatic carcinoma with necrosis consistent with breast primary. Tumor markers were ordered, and the pathology and cytology departments reported that estrogen-receptor (ER)/progesterone-receptor (PR) immunohistochemical assay results were ER-positive in 100% of nuclei and PR-negative. As per the surgical pathology department, this was stage IV cancer.
Using the Tyrer-Cuzick risk model, the patient’s lifetime risk of developing breast cancer was calculated at 1.5%, with no personal or first-degree family history of breast cancer. This also accounts for the lack of any BRCA mutations or other genetic mutations in the patient’s family. Despite her low risk, the patient nevertheless developed stage IV breast cancer, making this case unique in that it falls outside the normal risk range based on this generally used model to calculate the risk of breast cancer development.
The next day, the patient had developed increasing generalized muscle weakness, dehydration, poor oral intake of solids and liquids with severe nausea and vomiting, and worsening back pain. An oncologist was consulted and reviewed pathologic evaluation of biopsies and also sent biopsies of the bone marrow for evaluation. The oncologist’s preliminarily diagnosis was metastatic ER-positive, PR-negative, HER2/neu-negative, infiltrating ductal carcinoma of right breast.
Hypercalcemia correction was started with 60 mg (20 mL) of pamidronate disodium in 1000 mL (1 bag) of 0.9% sodium chloride intravenous therapy, infusing at 85 mL/h. Anastrozole 1 mg by mouth once daily was started for endocrine therapy. Postmenopausal women continue to produce low levels of estrogen from adrenal precursors that are converted to estradiol and estrone by aromatase in cancer cells.1 Anastrozole is a peripheral aromatase inhibitor designed to block the effect of estrogen on ER-positive receptors in cancer cells.
A computed tomography (CT) scan of the chest, abdomen, and pelvis without contrast was done to look for evidence of cancer progression. Findings showed numerous osteolytic lesions throughout the thoracic spine, ribs, and sternum, and numerous sclerotic lesions throughout the lumbar spine, sacrum, and pelvic bones, consistent with extensive metastatic disease (Figure 3). There was superior endplate depression of L5, L3, and L1 and kyphosis at T12-L1 with an uncommon presentation of a Schmorl node (intravertebral disk herniation).
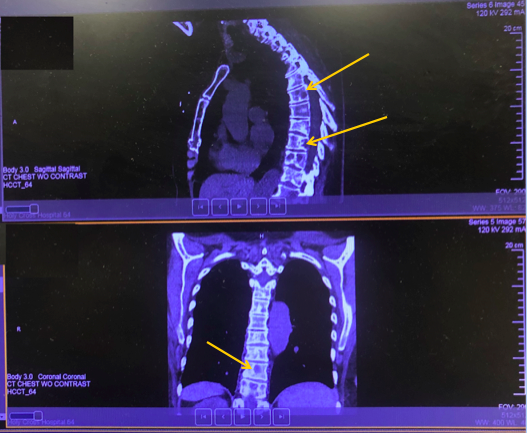
Figure 3. CT scan showed numerous osteolytic lesions throughout the thoracic spine, ribs, and sternum, and numerous sclerotic lesions throughout the lumbar spine, sacrum, and pelvic bones, consistent with extensive metastatic disease. There was superior endplate depression of L5, L3, and L1 and kyphosis at T12-L1 with an uncommon presentation of a Schmorl node.
Magnetic resonance imaging (MRI) of the total spine without contrast was also performed. Results showed diffuse abnormal low T1 bone marrow signal with heterogeneous T2 signal, findings consistent with extensive metastatic disease (Figure 4). Metastatic lesions were demonstrated in the thoracic and lumbar spine with minimal posterior bowing of cortex at T6, T9, and L1. Multilevel degenerative changes in the cervical spine contributed to multilevel spinal canal and neuroforaminal stenosis.
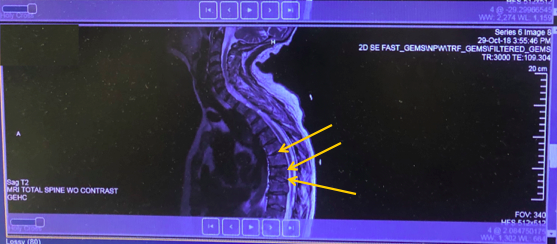
Figure 4. MRI of the total spine without contrast showed diffuse abnormal low T1 bone marrow signal with heterogeneous T2 signal, findings consistent with extensive metastatic disease. Metastatic lesions were demonstrated in the thoracic and lumbar spine with minimal posterior bowing of cortex at T6, T9, and L1.
On the following day, 1 unit of leukoreduced Rh-positive type O was transfused as a life-saving measure for severe anemia with a hemoglobin level of 6.6 g/dL. Bone marrow biopsies returned positive for spread of cancer to the marrow, which had caused the hemoglobin level to drop. Pamidronate in 0.9% sodium chloride was discontinued, and 1 dose of calcitonin salmon nasal was started to continue calcium correction.
The final diagnosis was stage IV breast cancer with bone marrow involvements/osteolytic bony metastasis and a spine lesion, with right breast biopsy showing infiltrative ductal grade 2 of 3. Immunohistochemical pathological assay results demonstrated ER positivity, PR negativity, and HER-2/neu negativity.
OUTCOME OF THE CASE
The patient progressively weakened despite chemotherapy. She was discharged and is in hospice care, with a do-not-resuscitate order as per her family. She was on oral anastrozole, 1 mg daily, palliative chemotherapy with palbociclib, 100 mg daily; and zoledronic acid, 4 g intravenously every 12 weeks The patient did not respond to chemotherapy as expected, and the prognosis was extremely poor due to the high stage, high grade, and late detection. Palliative measures were continued with pain control with fentanyl, 75 µg patch every 72 hours in the hospice setting. The patient died 12 days after discharge due to complications arising from disseminated intravascular coagulation. The 30-day survival rate in such cases has been reported as less than 50%.
DISCUSSION
Three major mechanisms by which hypercalcemia can occur are secondary to tumor secretion of parathyroid hormone–related protein (PTHrP), osteolytic metastases with local release of cytokines (including osteoclast-activating factors), and tumor production of 1,25-dihydoxyvitamin D (calcitriol). Hypercalcemia of malignancy due to osteolysis-induced local tumor-cell secretion of osteoclast-activating cytokines accounts for only 20% of all cases of hypercalcemia associated with malignancy.2
PTHrP is expressed by breast cancer cells in bone more often than cells in soft tissue or in the primary tumor. It acts locally to cause osteolysis. In patients with breast cancer, bone metastases, and hypercalcemia, serum PTHrP is elevated. However, osteolysis can still occur in the absence of high serum PTHrP.2 Interleukin 1 (IL-1), IL-6, and tumor necrosis factor α secreted by the tumor cells induce secretion of receptor activator of nuclear factor κΒ ligand (RANKL) by osteoblasts, stimulating osteoclastic differentiation and ultimately resorption of the bone.2 Surrounding production of osteoprotegrin, which normally inhibits RANKL, decreases.2 The estimated yearly prevalence of hypercalcemia for all cancers is 1.46% to 2.74%.3
On the molecular level, the cyclin-dependent kinases CDK4 and CDK6 pathway has been found to be overactive in breast cancer. CDK4/6 inhibition leads to activation of the retinoblastoma (Rb) tumor suppressor, causing cell-cycle arrest.4 Palbociclib is a reversible, small-molecule, selective inhibitor of CDK4 and CDK6.4 CDKs have a role in regulating progression through cell cycle at the G1/S phase by blocking Rb hyperphosphorylation.5 Palbociclib reduces proliferation of breast cancer cell lines by preventing progression from G1 to S20 phases of the cell cycle. The combination of palbociclib with anastrozole provides for increased inhibition of Rb phosphorylation, downstream signaling, and tumor growth compared with either agent alone.6 Even with these chemotherapeutic agents, 30% to 40% of metastatic ER-positive breast cancers have activating mutations in the estrogen-binding domain of the gene that encodes for ER receptors, dampening the prognosis with chemotherapy.7
Palbociclib was approved by the Food and Drug Administration based upon a phase 3 study that included 666 postmenopausal patients with metastatic, ER-positive, HER2-negative breast cancer who had not had prior treatment for advanced disease.8
- Ma CX. Treatment approach to metastatic hormone receptor-positive, HER2-negative breast cancer: endocrine therapy and targeted agents. UpToDate. https://www.uptodate.com/contents/treatment-approach-to-metastatic-hormone-receptor-positive-her2-negative-breast-cancer-endocrine-therapy-and-targeted-agents. Updated November 27, 2018. Accessed February 15, 2019.
- Hortwitz MJ. Hypercalcemia of Malignancy: mechanisms. UpToDate. https://www.uptodate.com/contents/hypercalcemia-of-malignancy-mechanisms. Updated May 22, 2018. Accessed February 15, 2019.
- Goldner W. Cancer-related hypercalcemia. J Oncol Pract. 2016;12(5):426-432.
- Kwapisz D. Cyclin-dependent kinase 4/6 inhibitors in breast cancer: palbociclib, ribociclib, and abemaciclib. Breast Cancer Res Treat. 2017;166(1):41-5
- Reagan P, Pani A, Rosner MH. Approach to diagnosis and treatment of hypercalcemia in a patient with malignancy. Am J Kidney Dis. 2014;63(1):141-147.
- Wright JD, Tergas AI, Ananth CV, et al. Quality and outcomes of treatment of hypercalcemia of malignancy. Cancer Invest. 2015;33(8):331-339.
- Pi J, Kang Y, Smith M, Earl M, Norigian Z, McBride A. A review in the treatment of oncologic emergencies. J Oncol Pharm Pract. 2016;22(4):625-638.
- Jalloh M. Palbociclib: a new breakthrough for advanced breast cancer. Pharmacy Today. https://www.pharmacist.com/article/palbociclib-new-breakthrough-advanced-breast-cancer. Published April 1, 2015. Accessed February 15, 2019.