
Peer Reviewed
Esophageal Stricture Secondary to Gastroesophageal Reflux Disease in a 2-Year-Old Boy
Authors:
Daniel Mannina, BSc
Schulich School of Medicine & Dentistry, Western University, London, Ontario, Canada
Roli R. Agrawal, MD
Windsor Regional Hospital Metropolitan Campus, Windsor, Ontario, Canada
Citation:
Mannina D, Agrawal RR. Esophageal stricture secondary to gastroesophageal reflux disease in a 2-year-old boy [published online December 19, 2018]. Gastroenterology Consultant.
A 2-year-old boy presented to the emergency department (ED) with significant failure to thrive and nonbloody, nonbilious vomiting.
History. The boy had been experiencing emesis with each meal and was only able to tolerate fluids. This had begun when the child was 2 weeks of age. There was no diarrhea, he was afebrile, he did not have any sick contacts and there were no infectious symptoms. He had recently immigrated to Canada with his family and had not received health care prior to arrival. He reportedly had been vaccinated at the time of immigration, but documentation was not available. Prenatal and birth history was not obtained. He had since been followed by a local pediatrician.
Prior to this ED visit, the patient had undergone 2 abdominal ultrasonography studies, the results of which were unremarkable. Additionally, 2 concomitant double-contrast upper gastrointestinal (GI) tract studies were attempted, but the patient was unable to tolerate the barium.
Physical examination. On examination, the patient appeared fatigued. He was tachycardic; all other vital signs were within normal limits. His abdomen was soft, nontender, and nondistended, and no masses were palpated. The remainder of the physical examination findings were normal.
Diagnostic tests. Laboratory test results were largely unremarkable except for microcytosis, with a mean corpuscular volume of 67 µm3. A liver function panel was performed, the results of which were normal. Additionally, electrolytes and creatinine levels were within normal limits.
Subsequently, the boy successfully underwent a double-contrast upper GI study (Figures 1 and 2). An esophageal stricture was identified involving the lower one-third of the esophagus. The esophagus was foreshortened, with a moderate-sized hiatal hernia secondary to traction. Proximal esophageal dilatation was present. No gastroesophageal reflux (GER) was noted during examination; however, the findings were in keeping with chronic/recurrent longstanding GER with secondary esophageal stricture.

Figure 1. Upper GI series with barium contrast, lateral view. An irregular stricture is visible in the distal esophagus. Proximal dilation and a mildly foreshortened esophagus is evident. A hiatal hernia secondary to traction is visible. The intrathoracic gastroesophageal junction is indicated by the black arrow.
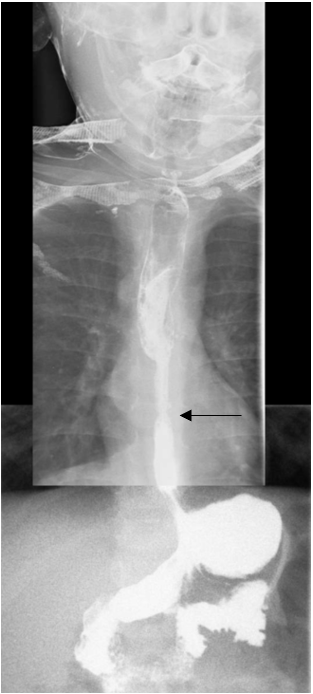
Figure 2. Upper GI series with barium contrast, anteroposterior view. The irregular stricture is again visible in the distal esophagus. Proximal dilation and a mildly foreshortened esophagus is evident. A hiatal hernia secondary to traction is visible. The intrathoracic gastroesophageal junction is indicated by the black arrow.
With this information, the child was referred to a pediatric surgery for evaluation. Gastroenterology and surgery together evaluated the patient. The boy underwent an esophagogastroduodenoscopy (EGD), during which a peptic stricture was identified and subsequently dilated. Biopsies of the proximal and distal esophagus were taken, which showed chronic nonspecific ulceration of the distal esophagus on pathology results. The proximal esophagus demonstrated normal histologic findings.
Treatment. Proton-pump inhibitor (PPI) therapy was then initiated for 4 months. The patient improved but presented to the hospital again 3 months later with vomiting. A repeat EGD was performed, which made note of the foreshortened esophagus, hiatal hernia, a mild circumferential narrowing proximal to the lower esophageal sphincter, and severe esophagitis. The PPI dosage subsequently was increased.
A third EGD was performed 1 month later, the results of which showed marked improvement of the esophagitis. Biopsy of the duodenum did not identify any pathologic abnormality. Stomach biopsy results were normal and were negative for Helicobacter pylori infection. A biopsy taken from the esophagus demonstrated mild esophagitis consistent with gastroesophageal reflux disease (GERD). He was subsequently seen in follow up by the gastroenterologist.
Outcome of the case. The patient was still experiencing occasional vomiting, but much less than at the time of his initial presentation. Moreover, he was gaining weight appropriately. Surgical intervention has not been required.
Discussion. Feeding difficulties and dysphagia in children are challenging problems requiring a broad differential diagnosis. Moreover, if a child is failing to thrive, it is imperative that these problems are corrected swiftly to mitigate potential long-term sequelae. To investigate the underlying cause, a systematic pathophysiologic approach should be employed, considering conditions that could lead to impairment of caloric intake, inadequate absorption, increased metabolism, or defective utilization of nutrients. Most commonly, failure to thrive is seen with inadequate caloric intake; thus, a detailed history of feeding and eating habits should be elicited to rule out nonorganic causes.1
If feeding habits and diet are determined to be appropriate, inadequate intake can be a result of central nervous system deficits leading to swallowing dysfunction; orofacial structural anomalies (eg, cleft palate or cleft lip); significant reflux; or structural disorders of the esophagus.1 Abnormalities that can lead to inadequate absorption include food allergies, celiac disease, cow’s milk allergy, or other food allergies. Potential causes for increased metabolism include congenital anomalies (heart and bronchopulmonary defects leading to chronic hypoxemia), chronic infection, and hyperthyroidism.1 Genetic abnormalities or metabolic disorders can lead to defective utilization of nutrients.
GER is common in infants. Approximately two-thirds of infants up to 4 months of age experience recurrent reflux or spitting up; this decreases markedly by 1 year of age and is largely absent by 18 months.2 However, it may be pathologic in some individuals and is thus referred to as GERD.
GERD may lead to poor weight gain, esophagitis, and respiratory distress (including apnea), or aspiration and subsequent pneumonia, or the child may become irritable with feeding or refuse feedings. In patients with these symptoms or with biopsy-confirmed esophagitis, pharmacotherapy with a PPI is trialed. If left untreated, esophageal stricture may develop due to recurrent GER and inflammation of the esophagus.
The child in our case had been born in a region of civil unrest and with limited health care access; as a result, his GERD remained undiagnosed for a significant time. As a result of his longstanding GERD, the child developed an esophageal stricture that was identified by way of an upper GI series and EGD.
Identifying whether the stenotic region is congenital or acquired is a vital consideration for further management. In addition to GERD, acquired stenosis may be due to a foreign body or ingestion of a corrosive substance. Conversely, congenital esophageal stenosis (CES) is a rare condition occurring in approximately 1 in 25,000 to 1 in 50,000 live births worldwide.3 CES has been defined as an intrinsic stenosis of the esophagus present at birth that is associated with congenital malformation of the esophageal wall architecture.3 Depending on the etiology, endoscopic and surgical management are the mainstays of treatment.3 Diagnosis requires a high index of clinical suspicion; presenting symptoms are often attributed to strictures secondary to GERD.
Our patient underwent endoscopic dilation of the stenotic region and PPI therapy. One of the hallmarks of CES is dysphagia that presents with the introduction of solid food into the infant’s diet. However, our patient developed feeding difficulties shortly after birth, which is in keeping with GERD and subsequent stenosis as opposed to CES. Together with the clinical history, EGD findings corroborated that the child had developed an esophageal stricture secondary to GERD. Ultimately, this highlights the broad differential diagnosis associated with failure to thrive and exemplifies the necessity of thorough workup to correct the underlying conditions.
- Jeong SJ. Nutritional approach to failure to thrive. Korean J Pediatr. 2011;54(7):277-28
- Campanozzi A, Boccia G, Pensabene L, et al. Prevalence and natural history of gastroesophageal reflux: pediatric prospective survey. Pediatrics. 2009;123(3):779-783.
- Kurian JJ, Jehangir S, Varghese IT, Thomas RJ, Mathai J, Karl S. Clinical profile and management options of children with congenital esophageal stenosis: a single center experience. J Indian Assoc Pediatr Surg. 2016;21(3):106-109.