
Peer Reviewed
Brain Abscess in a 5-Year-Old Girl
Authors:
Jonathan Frommelt, MD
Assistant Professor, Case Western Reserve University, and Attending Physician, Department of Emergency Medicine, MetroHealth Medical Center, Cleveland, Ohio
David Effron, MD
Associate Professor, Case Western Reserve University and Attending Physician, Department of Emergency Medicine, MetroHealth Medical Center, Cleveland, Ohio.
Citation:
Frommelt J, Effron D. Brain abscess in a 5-year-old girl [published online August 12, 2019]. Consultant360.
While on vacation out of town, a 5-year-old girl presented to an urgent care center with her parents out of concern for nausea and vomiting for the last 3 days and a change in behavior. The patient had last been well approximately 2 weeks prior, when she had developed a low-grade fever, headache, and intermittent nonbloody and nonbilious emesis. The family reported that the girl’s condition had improved with antipyretics, and strep pharyngitis was diagnosed at the urgent care center after a positive swab test. She was discharged with a prescription for amoxicillin after having tolerated an oral challenge.
At that time, the girl’s mother had expressed her concerns about the diagnosis, given that the patient had never reported having a sore throat, but after some reassurance the mother ultimately went along with the plan for antibiotics and close follow-up with a pediatrician in 1 to 3 days. Over the next 48 hours, the parents noticed that the fever had resolved and that their daughter was more playful and had resumed her normal daily activities and diet. Their follow-up visit at a pediatrician’s office the next day was described as uneventful.
Over the following week, after having returned home from vacation, the girl had lingering symptoms of mild frontal headaches and nausea, which continued to wax and wane despite her having completed the course of antibiotics. Mounting concerns for the patient’s well-being prompted a visit to the emergency department (ED).
On arrival to the ED, the family reported that the girl had had progressively worsening lethargy over several hours, worsening headaches, frequent emesis, and an episode of clenched fists with associated confusion and decreased responsiveness.
Review of systems in the ED revealed activity change, lethargy, appetite change, fever, nausea, vomiting, headache, confusion, and clenched fists. The patient’s mother denied any known vision changes, diplopia, eye redness, facial droop, slurred speech, neck stiffness, chest pain, abdominal pain, back pain, dysuria, rash, and leg swelling in the girl.
Physical examination demonstrated a temperature of 37°C, a heart rate of 130 beats/min, a respiratory rate of 20 breaths/min, and oxygen saturation of 96% on room air. She weighed 16.6 kg. The child was ill-appearing, lying in the fetal position with her eyes closed, easily arousable but moaning.
There was mild erythema to the posterior pharynx without asymmetry, exudates, or stridor, and shotty lymphadenopathy. Examination of the neck did not demonstrate any meningismus, but the child was agitated with neck range of motion. Cardiac, pulmonary, and abdominal examination findings were unremarkable, and no rash was present. Neurologic examination findings were negative for any cranial nerve, reflex, motor, or sensory deficits.
Laboratory test results in the ED demonstrated a leukocytosis (white blood cell count, 20,600/µL with 88% neutrophils) with a left shift, an erythrocyte sedimentation rate of 40 mm/h, a C-reactive protein level of 1.7 mg/L, and normal levels of electrolytes.
The history and physical examination prompted a computed tomography (CT) scan of the head without contrast, findings of which were concerning for a right temporoparietal mass or abscess (Figure 1).
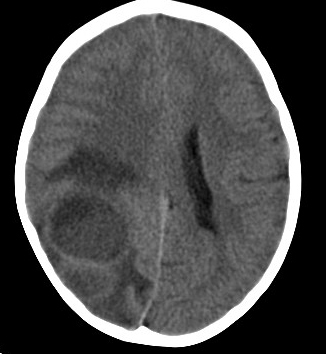
Figure 1. Noncontrast CT scan of the head showed an area concerning for a right temporoparietal mass or abscess.
A consulting neurosurgeon recommended a stat magnetic resonance imaging (MRI) scan, the results of which demonstrated a ring-enhancing lesion involving the right parieto-occipital region with restricted diffusion and marked surrounding edema, findings most consistent with pyogenic abscess (Figures 2 and 3).

Figure 2. T1-weighted MRI scan showed a ring-enhancing lesion involving the right parieto-occipital region with restricted diffusion and marked surrounding edema.

Figure 3. Fluid-attenuated inversion recovery MRI scan showed a ring-enhancing lesion involving the right parieto-occipital region with restricted diffusion and marked surrounding edema.
Broad-spectrum antibiotics (vancomycin and ceftriaxone) and antiepileptics (levetiracetam) were initiated, and the patient was taken emergently to the operating room for neurosurgical decompression.
In the operating room, a right-sided burr-hole craniotomy was performed with stereotactic aspiration, and 38 mL of pus was removed. Gram stain was positive for cocci in pairs and chains, and subsequent speciation showed Streptococcus mitis, which is normally found in the nasopharynx, mouth, and throat.
Postoperatively in the pediatric intensive care unit, the parents reported a history of an atrial septal defect, which was being followed with serial echocardiograms by the girl’s pediatrician and cardiologist. Furthermore, the patient had had dental work performed approximately 2 weeks prior to symptom onset, making hematogenous spread the most likely cause of infection. Inpatient echocardiography findings did not show valvular vegetation but did demonstrate a known left-to-right atrial shunt.
The patient had an uncomplicated postoperative course. She was extubated immediately after her procedure and remained neurologically intact without focal deficits or recurrent seizures throughout her hospital course. She was discharged 5 days later with a peripherally inserted central catheter for extended outpatient intravenous antibiotics for 100 days and scheduled outpatient follow-up with a neurosurgeon and her pediatrician.
DISCUSSION
Brain abscesses begin as a focal cerebritis that evolves into a dynamic encapsulated collection of intracranial pus that poses a life-threatening emergency. Once universally fatal, modern advances in neuroimaging, neurosurgical technique, and newer broad-spectrum antibiotics have drastically altered morbidity and mortality. A recent meta-analysis indicates a decreased fatality rate from 40% to just 10% and full recovery in up to 70% of patients.1,2 Despite these advancements and recent trends, morbidity remains high, with major long-term complications including seizures (up to 80%),3 persistent mental status change, and focal neurologic deficits. Immunocompromised patients (especially those with organ transplants and HIV infection) have an increased incidence of brain abscess.
Brain abscesses occur by way of 3 main mechanisms: spread from contiguous pericranial infections, hematogenous spread from a distal source, or through direct inoculation. Common contiguous sources include sinusitis, otitis, and odontogenic infections, all of which comprise 25% to 50% of all cases.1,3-6 Lung abscess, empyema, endocarditis, soft tissue infections, and intra-abdominal infections allow for hematogenous spread and are responsible for 15% to 30% of cases.1,3,7,8 Congenital heart disease, including patent foramen ovale and pulmonary arteriovenous fistula, may predispose in instances where no clear source is found, which occurs 20% to 40% of the time.3 The remaining 8% to 19% occur through either traumatic events or neurosurgical procedures.3
Streptococcus and Staphylococcus are the most commonly isolated microorganisms, with Streptococcus constituting the vast majority of isolates (nearly 70%).1,2,9 Staphylococcus is significantly more common in traumatic or neurosurgical cases, but gram-negative rods such as Pseudomonas, Klebsiella, Escherichia, and Proteus can also be seen in this setting. Opportunistic infections such as with Pseudomonas, Toxoplasma, Listeria, Nocardia, Aspergillus, Cryptococcus, Coccidioides, and other fungal pathogens should be considered in patients with HIV/AIDS, alcoholism, chronic steroid or immunosuppressant therapy, and debilitating neurologic disease (eg, Alzheimer disease, Parkinson disease). Although cases are rare, immigrant populations have increased risk of parasitic infections such as cysticercosis, Entamoeba histolytica, and schistosomiasis, as well.2,6,9,10
Clinical presentation of a brain abscess varies greatly due to an extraordinary number of variables. The organism’s pathogenicity, site size and number of infectious lesions, specific brain structures affected, and nearby neuroanatomy that may be affected by edema, mass effect, or local destructive effects all contribute to the clinical picture. Clinicians must keep in mind the possibility of secondary cerebral injuries, as well.
Despite all of this, brain abscesses typically present with 1 of 4 basic syndromes: elevated intracranial pressure, focal mass effect, a focal neurologic deficit, or diffuse destruction and coma. Reported symptoms are usually fever, headache, altered mentation, focal neurologic deficit, seizure, nausea and vomiting, or some combination thereof, with headache being the most common presenting symptom (72%-92% of cases).2,3 Fever is the next commonest symptom but may only be present in less than 50% of cases, according to the most recent meta-analysis.2,3,11 Meningismus is present in approximately half of all cases, and nausea and vomiting in one third.2,3 Interestingly, seizures are only present in 20% to 25% of cases at onset despite being present in up to 80% of patients after diagnosis and treatment.2,3 The duration of these symptoms is often indolent, lasting 10 to 11 days on average but possibly as long as 2 to 8 weeks.2 Mental status or level of consciousness varies widely as indicated by assessment with the Glasgow coma scale (GCS) on hospital admission: GCS score of 3 to 8, approximately 10%; GCS score of 9 to 12, approximately 28%; and GCS score of 13 to 15, approximately 62% of cases.2,3 No focal neurologic deficit may be appreciable in nearly 40% of cases, as well.2
Diagnosis is typically made with a high index of clinical suspicion and prompt neuroimaging. Laboratory test results may suggest infection or inflammation but are otherwise nonspecific. Lumbar puncture (LP) should never be performed if brain abscess is suspected, since it does not aid in diagnosis and may result in herniation secondary to increased intracranial pressure. This was highlighted by a recent meta-analysis that retrospectively reported that LP had been performed in nearly 20% of included cases.12 Of these, 26 patients had significant clinical deterioration, and 7 patients died.12 In the ED, CT scan is the test of choice given its short duration and ease of availability, but MRI may be required for further characterization, since it is more sensitive and may better differentiate neoplasms from ring-enhancing lesions.
Treatment is primarily surgical decompression, which highlights the need for prompt recognition and neurosurgical consult. Surgery is both therapeutic, relieving mass effect or elevated intracranial pressure, and diagnostic, helping isolate the causative agent. Empiric antibiotics should be broad-spectrum and cross the blood-brain barrier in sufficient concentrations, as well as cover for anaerobic pathogens. Therefore, ceftriaxone and metronidazole are the drugs of choice in this instance. Vancomycin should be added for penetrating trauma or recent neurosurgery. Specific immunodeficient populations require special consideration. Antibiotic therapy alone may be considered in patients with multiple abscesses, single small abscess of less than 2.5 cm, and GCS score greater than 13, or if the pathogen has already been isolated with a GCS score greater than 13.2,6 This decision should be made in concert with a neurosurgeon. Length of treatment typically ranges from 4 to 8 weeks depending on whether surgery is undertaken or not.
There are no good data supporting concomitant corticosteroid therapy, with the exception of perioperatively in the face of cerebral edema and impending herniation. Antiepileptic medication initiation and length of treatment is variable, but most recommend at least 3 months of seizure prophylaxis, and electroencephalography should be utilized to help guide decisions to maintain or cease therapy.3,6 The antiepileptic drug of choice in children is phenytoin given as 15 to 20 mg/kg IV acutely and transitioned to oral therapy before hospital discharge.
The prognosis depends on several factors but is generally poorer for newborns and the elderly. The rate of progression and GCS score at admission correlate directly with the mortality rate. Poor prognosticators include delayed diagnosis, rapid progression, posterior fossa location, multiple lesions, interventricular rupture, fungal etiology, and coma. Mortality can be as high as 80% with interventricular rupture or posterior fossa locale.1,10,11
- Brouwer MC, Coutinho JM, van de Beek D. Clinical characteristics and outcome of brain abscess: systematic review and meta-analysis. Neurology. 2014;82(9):806-813.
- George N, Siket SS. Brain abscess in emergency medicine. Medscape. https://emedicine.medscape.com/article/781021-overview. Updated May 18, 2017. Accessed August 12, 2019.
- Alvis Miranda H, Castellar-Leones SM, Elzain MA, Moscote-Salazar LR. Brain abscess: current management. J Neurosci Rural Pract. 2013;4(suppl 1):S67-S81.
- Carpenter J, Stapleton S, Holliman R. Retrospective analysis of 49 cases of brain abscess and review of the literature. Eur J Clin Microbiol Infect Dis. 2007;26(1):1-11.
- Loeser E Jr, Scheinberg L. Brain abscesses: a review of ninety-nine cases. Neurology. 1957;7(9):601-609.
- Southwick F. Pathogenesis, clinical manifestations, and diagnosis of brain abscess. UpToDate. https://www.uptodate.com/contents/pathogenesis-clinical-manifestations-and-diagnosis-of-brain-abscess. Updated January 28, 2019. Accessed August 12, 2019.
- Horiuchi Y, Kato Y, Dembo T, Takeda H, Fukuoka T, Tanahashi N. Patent foramen ovale as a risk factor for cryptogenic brain abscess: case report and review of the literature. Intern Med. 2012;51(9):1111-1114.
- Kawamata T, Takeshita M, Ishizuka N, Hori T. Patent foramen ovale as a possible risk factor for cryptogenic brain abscess: report of two cases. Neurosurgery. 2001;49(1):204-206.
- Mace SE. Central nervous system infections as a cause of an altered mental status? What is the pathogen growing in your central nervous system? Emerg Med Clin North Am. 2010;28(3):535-570.
- Muzumdar D. Central nervous system infections and the neurosurgeon: a perspective. Int J Surg. 2011;9(2):113-116.
- Helweg-Larsen J, Astradsson A, Richhall H, Erdal J, Laursen A, Brennum J. Pyogenic brain abscess, a 15-year survey. BMC Infect Dis. 2012;12:332. doi:10.1186/1471-2334-12-332.
- Nathoo N, Nadvi SS, Narotam PK, van Dellen JR. Brain abscess: management and outcome analysis of a computed tomography era experience with 973 patients. World Neurosurg. 2011;75(5-6):716-726.