
Peer Reviewed
Palisaded Neutrophilic Granulomatous Dermatitis With Concomitant Leukocytoclastic Vasculitis: A Spectrum of a Rare Disease
Authors:
Alexander Mounts, DO, MA
US Naval Flight Surgeon, Naval Medical Center San Diego, California
Kristopher M. Peters, DO
Staff Dermatologist, Madigan Army Medical Center, Joint Base Lewis-McChord, Washington
Citation:
Mounts A, Peters KM. Palisaded neutrophilic granulomatous dermatitis with concomitant leukocytoclastic vasculitis: a spectrum of a rare disease [published online September 19, 2019]. Consultant360.
Disclaimer:
The views expressed in this article are those of the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.
A 55-year-old woman was referred to a dermatology practice for a cutaneous eruption over the elbows and posterior thighs of one month’s duration. The affected areas had been intensely pruritic, with minimal improvement with the use of diphenhydramine. She had a 15-year history of worsening rheumatoid arthritis (RA), which was being managed with oral prednisone and oxycodone-acetaminophen.
Physical examination revealed several nontender skin-colored to erythematous papules with peripheral scale on the extensor surface of the bilateral elbows (Figure 1). Nonblanching, nontender, well-defined, annular purpuric papules and coalesced plaques were present on the posterior thighs (Figure 2).

Figure 1. Nontender erythematous to skin-colored scaling papules on the dorsal elbows.

Figure 2. Nonblanching well-defined non-tender purpuric plaques covering most of the bilateral lateral posterior thighs.
A punch biopsy of a lesion on the left arm demonstrated palisaded neutrophilic granulomatous dermatitis (PNGD) (Figures 3 and 4), and a punch biopsy of a lesion on the right thigh demonstrated small vessel vasculitis.

Figure 3. Palisaded granulomas surrounding leukocytoclastic debris and altered collagen.
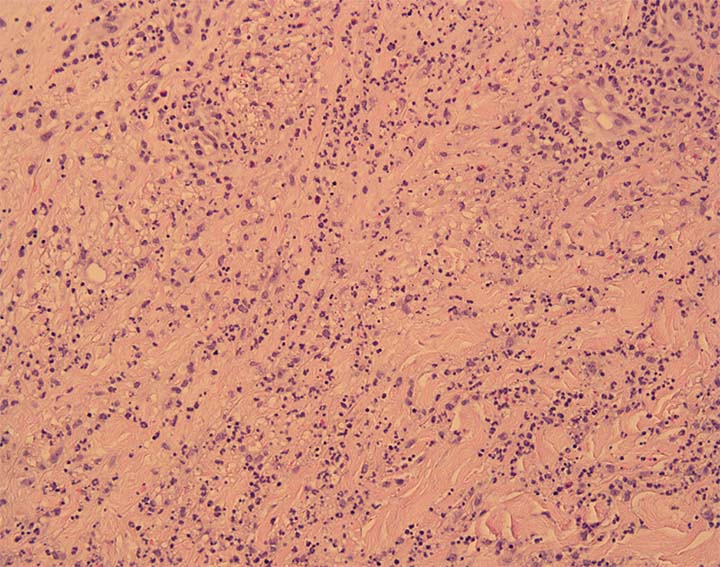
Figure 4. On higher magnification, numerous neutrophils and neutrophilic debris comprise the inflammatory infiltrate.
The patient was treated symptomatically for the pruritus with triamcinolone ointment, 0.1%, and cetirizine, 10 mg daily, until she was able to return to her rheumatologist for more aggressive management of her underlying RA. She had significant improvement of her skin lesions with this treatment regimen before she was ultimately switched to etanercept by her rheumatologist, after which her lesions resolved entirely.
DISCUSSION
Palisaded neutrophilic granulomatous dermatitis (PNGD) is a rare dermatologic condition that presents as a continuum of heterogeneous stages. Due to its many stages, it has been hard to define PNGD clinically and histopathologically. There has been much overlap with other conditions such as interstitial granulomatous dermatitis (IGD) and interstitial granulomatous drug reaction (IGDR).1 Depending on the literature, these different conditions have been viewed as the same disease, subsets of the same disease, or totally distinct processes.
PNGD has been associated closely with many systemic conditions and has only rarely been seen in the absence of any other disease processes. It is most commonly seen in association with connective tissue diseases such as systemic lupus erythematous, RA, granulomatosis with polyangiitis, hematologic disorders, and rarely in reactions to infections or medications.1
PNGD typically affects only adults and is seen more frequently in women.1,2 This tendency may be attributed to the strong association of PNGD with systemic autoimmune diseases, which are more prevalent in women.2 The pathogenesis of PNGD has not been elucidated, but it has been suggested to begin as a leukocytoclastic vasculitis.3 The condition can last from a few months to a few years.4 Our patient presented with PNGD with concomitant leukocytoclastic vasculitis likely secondary to poorly managed RA.
Clinically, PNGD typically presents as skin-colored to erythematous papules distributed symmetrically on the extremities with an overlying ulceration and crust.4 PNGD has also been reported to appear as urticarial plaques, erythematous nodules, pink and red plaques, violaceous patches and plaques, annular papules and plaques, and linear bands.5
The histological presentation of PNGD differs depending on the stage at which the sample is obtained. Initially, dense neutrophilic infiltrates with or without leukocytoclastic vasculitis and degenerated collagen are seen. Biopsies taken from fully developed lesions show palisaded granulomas surrounding leukocytoclastic debris and altered collagen. Toward the end of its course and resolution, palisaded granulomas with dermal fibrosis and scant neutrophilic debris are seen.4
PNGD shares many characteristics with IGD and is considered by some to be a subset of the same disease process. IGD is typically characterized clinically by linear cords or bands of erythematous to violaceous patches and plaques, frequently found on the lateral trunk, proximal upper limbs, extensor surfaces, and axillae.6 Histologically it can appear similar, as well, with palisaded granulomatous patterns and degenerated collagen, but without any vasculitis present.3
The vasculitis found in PNGD is an important point, since it is theorized that the lesions are triggered by circulating immune complexes.3 The deposition of immune complexes leads to a leukocytoclastic vasculitis that evolves into the progressive histological and clinical processes seen in PNGD.2,7
Due to the vast array of associated diseases and possible triggers for PNGD, it is critical to have a thorough and expansive workup to identify possible culprits. In the evaluation of patients with concurrent systemic connective tissue disease, appropriate initial workup should include tests for antinuclear antibodies, antineutrophil cytoplasmic antibodies, rheumatoid factor (RF), and other clinically correlated markers. In patients with concurrent arthritis, tests for RF and cyclic citrullinated peptide antibodies and imaging studies should be obtained. If a malignancy is suspected, an age-appropriate malignancy screen should be obtained with a complete blood cell count with differential and serum and urine protein electrophoresis. In patients with possible drug-induced disease, a medication reconciliation of likely culprits such as calcium-channel blockers, β-blockers, angiotensin-converting enzyme inhibitors, and statins should be performed.1
Standard initial treatment consists of a skin biopsy and targeting of the underlying inciting condition. In most cases, which usually have an associated systemic autoimmune disease, initial treatment with systemic corticosteroids is standard. Other treatment options with some efficacy include colchicine, cyclosporine, cyclophosphamide, hydroxychloroquine, nonsteroidal anti-inflammatory drugs, and dapsone. In cases of drug-induced or infection-induced processes, removal of the offending agent or treatment of infection is key. A proportion of cases have also been seen to spontaneously resolve. In a review of 92 cases, 20% to 25% showed signs of spontaneous resolution.3 Recurrence of disease has been seen.2,8
Our patient’s clinical presentation was consistent with the various stages of PNGD, with leukocytoclastic vasculitis lesions on the lower extremities and the fully developed papular lesions on the elbows. She had excellent improvement with conservative topical management prior to gaining better control of her underlying RA. The history of a well-established cause of PNGD and complete resolution of skin lesions with better control of the RA obviated the need for further workup.
REFERENCES:
- Rosenbach M, English JC III. Reactive granulomatous dermatitis: a review of palisaded neutrophilic and granulomatous dermatitis, interstitial granulomatous dermatitis, interstitial granulomatous drug reaction, and a proposed reclassification. Dermatol Clin. 2015;33(3):373-387.
- Hantash BM, Chiang D, Kohler S, Fiorentino D. Palisaded neutrophilic and granulomatous dermatitis associated with limited systemic sclerosis. J Am Acad Dermatol. 2008;58(4):661-664.
- Misago N, Shinoda Y, Tago M, Narisawa Y. Palisaded neutrophilic granulomatous dermatitis with leukocytoclastic vasculitis in a patient without any underlying systemic disease detected to date. J Cutan Pathol. 2010;37(10):1092-1097.
- Al-Daraji WI, Coulson IH, Howat AJ. Palisaded neutrophilic and granulomatous dermatitis. Clin Exp Dermatol. 2005;30(5):578-579.
- Stephenson SR, Campbell SM, Drew GS, Magro CM. Palisaded neutrophilic and granulomatous dermatitis presenting in a patient with rheumatoid arthritis on adalimumab. J Cutan Pathol. 2011;38(8):644-648.
- Sangueza OP, Caudell MD, Mengesha YM, et al. Palisaded neutrophilic granulomatous dermatitis in rheumatoid arthritis. J Am Acad Dermatol. 2002;47(2):251-257.
- Chu P, Connolly MK, LeBoit PE. The histopathologic spectrum of palisaded neutrophilic and granulomatous dermatitis in patients with collagen vascular disease. Arch Dermatol. 1994;130(10):1278-1283.
- Bremner R, Simpson E, White CR, Morrison L, Deodhar A. Palisaded neutrophilic and granulomatous dermatitis: an unusual cutaneous manifestation of immune-mediated disorders. Semin Arthritis Rheum. 2004;34(3):610-616.