
Effects of Yoga in Older Adults with Chronic Health Conditions: A Critical Review
Authors: Corjena Cheung, PhD, RN; Juyoung Park, PhD; Jean F. Wyman, PhD, RN
Although yoga is commonly taught in gyms, health clubs, community centers, and colleges as an exercise option, there has been an increasing interest in the therapeutic use of yoga to prevent and treat chronic health conditions in the past decade. Yoga is classified as a mind-body practice by the National Center of Complementary and Alternative Medicine, with its origins in ancient Indian philosophy.1 Yoga is a discipline that is divided into many branches. Hatha yoga, the physical practice of yoga, is the most common form in North America. It encompasses nearly all types of modern yoga such as Iyengar yoga, a gentler form of yoga that allows for individual variation in the ability of participants and specifically includes the use of assistive devices such as blocks, belts, and blankets to support parts of the body while performing the poses. The various types of Hatha yoga that people use for health purposes typically combine physical postures (asanas), breathing techniques (pranayama), and meditation or relaxation. The postures are done sequentially with the purpose of promoting flexibility and strength. Some suggest that the bending, twisting, and stretching movements also massage the internal organs and glands.2 The breathing and meditation exercises are intended to calm and focus the mind and to develop deeper level of concentration and greater self-awareness.3
With normal aging and accumulation of chronic health conditions, older adults are at increased risk of disability, diminished quality of life (QOL) and increased costs for healthcare and long-term care.4 About 80% of older adults have one chronic condition. Treating patients with chronic diseases accounts for 75% of the nation's healthcare spending.5 Because many chronic health conditions are related to lifestyle, current physical activity and exercise guidelines for older adults recommend that exercise is a means to maintain health and preserve functional independence in old age.6 Yoga is a promising exercise option for older adults with chronic health conditions.7
A number of systematic literature reviews and meta-analyses indicate that yoga is a safe and effective intervention for chronic health problems such as low back pain,8 anxiety and depression,9 type 2 diabetes,10 and cancer.11 However, these studies focused mostly on adults younger than age 60, and results may not necessarily be transferable to the needs of older populations. Although yoga is generally considered to be safe when practiced appropriately in healthy individuals and that regular practice of yoga has been shown to benefit musculoskeletal and mental health conditions,9,10 evidence of yoga to be used safely and effectively in the older adult population has not yet been established.
According to a recent survey, of the 15.8 million American adults who reported that they were practicing yoga, 18.4% were age 55 years or older.12 The growing interest of older adults in yoga and the high prevalence of chronic health conditons in this population has led researchers to investigate the effects of yoga in older adults. In addition, unlike their younger counterparts, many older adults have chronic health conditions that affect their balance, physical strength, and feeling of security with physical activities that could impede their ability to participate in yoga practice.13,14 The need to critically examine the current evidence of yoga is timely for both healthcare consumers and providers.
The purpose of this literature review was to examine relevant studies on the effects of practicing yoga in older adults with chronic health problems, and to synthesize the findings to determine the evidence on whether the practice of yoga is safe and beneficial in older adults with chronic health conditions. The quality of methodology will be examined and summarized to help inform future research in this field.
________________________________________________________________________________________________________________________________________________________________
RELATED CONTENT
Exercise for Patients With Diabetic Peripheral Neuropathy
Yoga May Help Women Ease PTSD Symptoms
________________________________________________________________________________________________________________________________________________________________
Methods
A literature search was performed to identify existing peer-reviewed articles and dissertations published in English between January 2000 and February 2013 on the use of yoga in older adults with chronic health conditions. The following databases were used:
• Cochrane Databases of Systematic Reviews, Database of Abstracts of Reviews of Effects, Medline, CINAHL, PsychoINFO, and ProQuest Digital Dissertations;
• Symposium, conference and colloquium proceedings and abstracts;
• Internet search engine Google Scholar to identify gray literature;
• The list of references for each of the relevant studies;
• Bibliographies of relevant book chapters were hand-searched for further articles.
Various combinations of the key words such as “yoga,” “older adults,” “senior,” “elderly,” and “aged” were used in the search process.
Selection Criteria
Eligible studies included randomized controlled trials (RCTs) on a yoga intervention for a specific chronic health condition in older adults (age ≥60 years). Studies had to include physical and/or psychological outcome measures. Although “mindfulness meditation” is imbedded in yoga practice, for consistency and uniformity, such studies were excluded. Articles were also excluded if: (a) they were unavailable in English, (b) were published in non-peer-reviewed journals, (c) the mean age of the participants were less than 60 years, and (d) were not RCTs.
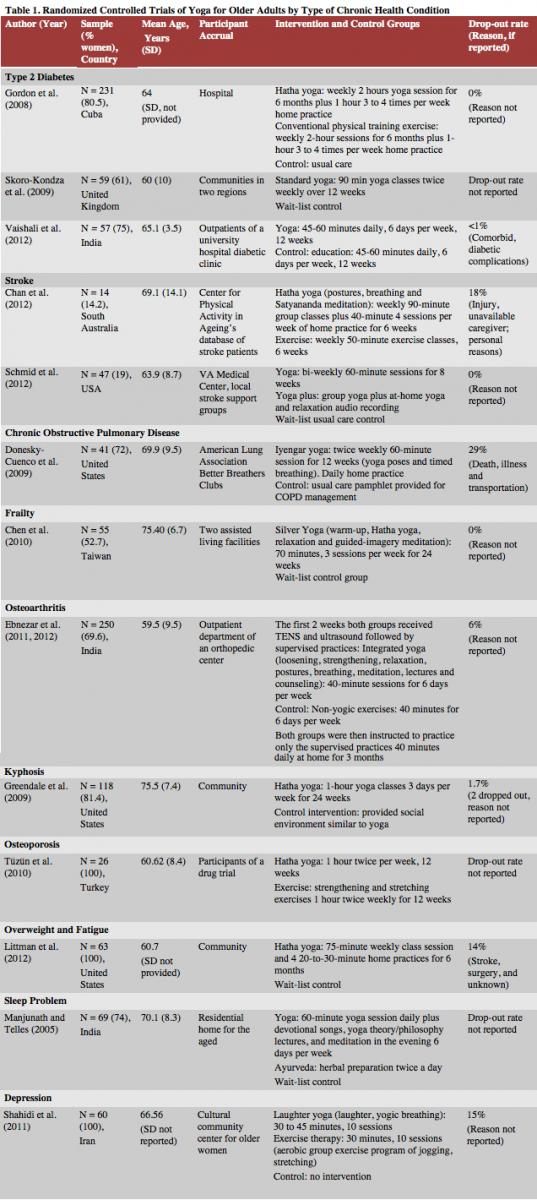
We (authors Cheung and Park) initially screened the titles and abstracts of all citations were initially screened against the inclusion/exclusion criteria. Any disagreements in study selection were resolved by discussion. Studies that were excluded in the screening process were recorded with reasons for exclusion. Data from selected articles were critically reviewed and extracted (Table 1).
Quality Assessment
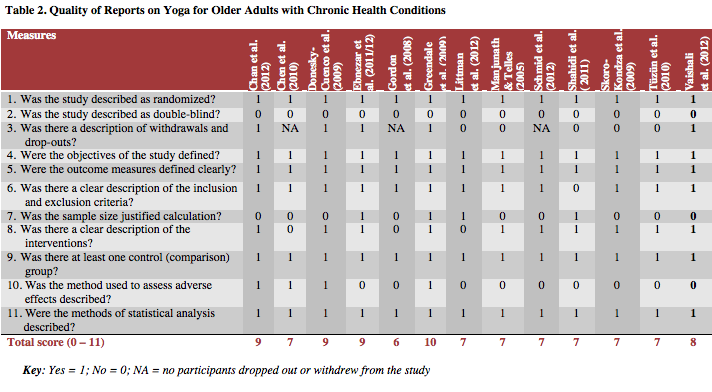
Both researchers independently performed the quality evaluation on all selected studies. Discrepancies on ratings were discussed and a consensus was reached. Studies were assessed using Jadad’s quality assessment checklist.15 This evaluation guideline is applicable to RCTs. It consists of 11 items with a maximum score of 11, which represents the highest quality (Table 2). The Jadad Quality Assessment scale is a widely used scale in healthcare studies and has well established psychometric properties.16
Results
Studies Identified
The search strategy generated a total of 258 articles, with 14 articles meeting the selection criteria. Two of the articles that reported different outcomes (physical symptoms versus quality of life) were based on the same study.17,18 A majority of studies were conducted in the Unites States,19-22 followed by India,17,18,23,24 Australia,25 Cuba,26 Iran,27 Taiwan,28 Turkey,29 and the United Kingdom.30
Study Quality
Although all studies were RCTs, none were double-blinded studies. Table 2 presents the outcome of the quality assessment. The quality score of each study ranged from 6 to 10 (maximum possible score of 11). Eight trials (62%) were of medium methodological quality (scored 4-7 on the Jadad scale) and 5 trials (38%) were of high quality (scored 8 or higher on the Jadad scale).
Design
Table 1 depicts the methodologies of 13 reviewed studies. All studies were RCTs with either 2 or 3 arms using convenience sampling methods except for 2 studies that used stratified24 or random samples.27 Only 2 studies17,18,30 included follow-up outcome measures to determine whether the effect of yoga was sustained after intervention was completed.
Participants
The mean age of participants' (n=1078, 75% female) was 66.3 ± 8.6 years, and they had a variety of chronic health conditions. The majority of participants resided independently in the community, with the exception of one study,27 which included residents in assisted living facilities.
Yoga Intervention
A variety of types, frequencies, and durations of yoga interventions were used in the studies reviewed. Hatha yoga was the most commonly type used.19,22,25,26,29 Four additional types and styles of yoga were studied: Iyengar yoga method20; integrated yoga, in which researchers included lectures and counseling on yogic concepts of health and disease17,18; researcher-developed Silver Yoga, which includes warm-up, Hatha yoga, relaxation, and guided-imagery meditation28; and laughter yoga, which combines unconditional laughter with yogic breathing.27 Four studies did not specify the type of yoga used.21,23,24,30 The frequency of the interventions ranged from once a week22,25,26 to 6 days per week.17,18,23,24 All studies involved group seesions. Only five studies included home practices as well.20-22,25,26 The duration of the interventions varied from 30 to 120 minutes per session for 6 to 24 weeks (Table 1). Longer duration and higher frequency of yoga intervention, and those that included approaches more than physical poses were commonly conducted in India.17,18,23,24
Yoga for Chronic Health Conditions
Diabetes. A total of three studies (n=347) examined yoga as a means to improve type 2 diabetes.23,26,30 These studies used a variety of intervention protocols (Table 1). All three studies incorporated postures, breathing, and relaxation techniques in the program, none included meditation. There was a low drop-out rate (<1%) reported in these studies.Two studies that examined physiological outcomes reported a significant improvement in A1C, fasting blood glucose, serum lipid profile, oxidative stress markers, and antioxidant status.23,26 The only study that examined both physiological (A1C and cardiovascular risk) and psychological measures (diabetes related quality of life and self-efficacy) found no significant change in any of the outcome measures but concluded that poor yoga exercise adherence and inadequate intensity and/or duration of yoga intervention might have contributed to the nonsignificant outcomes.30 None of the studies included any information on adverse events in their reports.
Stroke. Two studies were found that tested the effectiveness of yoga in post-stroke patients (n=61).21,25 Both studies used different yoga approaches and examined different outcome measures (Table 1). One study focused on the effect of yoga on improving balance21 and the other focused on relieving symptoms of depression and anxiety.25 Findings from the study that examined the psychological effects of yoga indicated that changes in depression and state and trait anxiety did not significantly differ between the treatment and control groups.25 However, program adherence was reported to be poor, with an 18% dropout rate due to injury, unavailable caregiver, and personal reasons. Results from the study that examined yoga’s effect on balance found a significant improvement on balance, and that all participants completed the intervention program.21No adverse events were reported in either study.
Chronic obstructive pulmonary disease (COPD). Only one study was located that compared the effect of yoga intervention in older patients with COPD versus a usual care control group.20 Yoga training significantly improved 6-minute walk31 distance and self-reported functional performance compared to usual care at the end of the program. However, no significant changes were found in depressive symptoms, anxiety, or general disease specific health-related QOL. Participants in the study reported difficulty with performing yoga independently at home. The study also suffered a high drop-out rate (29%). Researchers also noted that because the Iyengar yoga tradition considers breathing practice as an advanced technique to be practiced only after the poses are mastered; such technique was inadequately included to affect the physiological and psychological outcomes in this particular clinical population.
Frailty. A researcher-developed Silver Yoga exercise program was specifically designed for frail older adults.28 Residents of 2 assisted living facilities who had multiple chronic illnesses and were mildly functionally dependent were recruited. All physical fitness indicators of participants in the intervention group improved significantly at the end of the yoga program (Table 3).
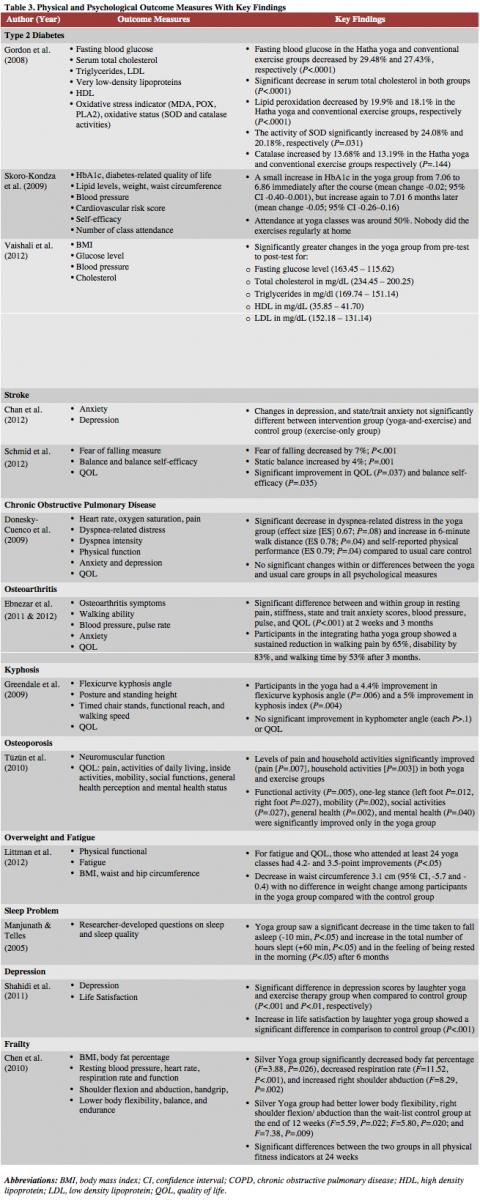
Musculoskeletal disorders. Three studies that assessed the effects of yoga for managing musculoskeletal disorders were included for review: osteoarthritis (OA),17,18 kyphosis,19 and osteoporosis.29 There was no consistency in the type of intervention protocols or yoga dose among these studies (Table 1). Only one of the three studies reported the method used to assess adverse effects (ie a monthly symptom checklist including possible side effects of the yoga intervention).19 Drop-out rate in the 3 studies ranged from 1.7%19 to 6.0%,17,18 but none of the studies reported reasons for dropouts. Therefore, it was not clear whether the dropout rate was associated with adverse events or injury due to the yoga intervention. Ebnezar et al17,18 compared the efficacy of integrated yoga therapy with non-yogic physiotherapy exercises for managing OA of the knee joint. They found that an integrated yoga therapy was better than non-yogic physiotherapy exercise when combined with transcutaneous electrical nerve stimulation (TENS) and ultrasound treatment for reducing walking pain, improving range of knee flexion, increasing walk time, and reducing tenderness, swelling, crepitus, and knee disability in older patients with OA. Participants in the integrated yoga group showed a sustained reduction in walking pain, disability, and walking time at 12 weeks follow-up.
The Greendale et al19 study assessed whether Hatha yoga improved thoracic kyphosis angle, posture, physical function, and QOL in older persons with hyperkyphosis. This study provided the longest duration (24 weeks) of yoga interventions among the three studies. Although participants in the yoga intervention experienced greater improvement in flexicurve kypohsis angle and kyphosis index than those in the control group, the intervention did not provide significant improvement in Debrunner Kypohmeter angle, physical performance, or health-related qualiy of life.
Tüzün et al29 compared the effect of yoga to a classic exercise program on balance and QOL in postmenopausal women with osteoporosis. In contrast to the classic exercise group, the yoga group had significant improvement in functional activity, one-leg stance, mobility, social activities, general health, and mental health. Levels of pain and household activities were significiantly improved in both groups.
Other chronic health conditions. Three studies examined different chronic health conditions in older adults: depression,27 sleep problems,24 and fatigue and overweight.20 The study by Shahidi et al27 was designed to compare the efficacy of laughter yoga (combination of unconditioned laughter and yogic breathing) and group exercise therapy versus a no treatment control group in decreasing depression and improving life satisfaction in older women diagnosed with depression. No difference was found between the laughter yoga and exercise therapy groups in reduction of depressive symptoms or improvement in life satisfaction scores, although there was a significant difference in decrease in Geriatric Depression Scale and Diener Life Satisfaction Scale scores in both the laughter yoga and exercise groups when compared to the control group.
Littman et al22 examined the effect of an intensive yoga program on fatigue, QOL, and weight change in breast cancer survivors. Participants who attended at least 24 yoga classes had significant improvements in fatigue and breast cancer related QOL, compared with those in the control group. Manjunath and Tellers24 compared the effects of yoga and Ayurveda on the quality of sleep in geriatric populations. The groups were evaluated for self-assessment of sleep during 1-week periods at baseline, 3 months, and 6 months. The yoga group showed signifcantly greater improvement in quality of sleep (time required to fall asleep, total hours of sleep, and feeling rested in the morning) than the other groups.
Discussion
This review addressed the effect of yoga practice on chronic health conditions that commonly affect the older population including type 2 diabetes, post-stroke, COPD, OA, osteoporosis, sleep disorders, depression, hyperkyphosis, and frailty. Practicing yoga was found to have consistent positive effects on physical health: improving blood glucose and cholesterol levels, balance, flexibility, muscle strength, flexicurve kypohsis angle and kyphosis index, sleep quality, joint stiffness, and joint pain. Findings on psychological health including anxiety, depression, and QOL are inconsistent. Although a few reports indicated that there were no adverse events associated with yoga practice, the lack of reporting of adverse events in most studies limited any conclusion regarding the safety of practicing yoga in a class or home setting.
Despite an extensive search of the literature using a number of databases including the gray literature, we could only locate 13 RCTs on yoga interventions with older adults for chronic health conditions. To locate high-quality RCTs, we excluded a number of single group pre-post trials. The majority of these trials were of moderate quality. Although it may not be feasible to use double blinding in exercise intervention studies, a majority of these studies included small sample sizes and did not provide power estimates.
In addition, this review indicated several limitations in the available evidence. First, yoga practice varied in type, frequency and duration among trials. Because there are many different types of yoga, yoga training, and philosophy, the diversity in yoga regimens prescribed was to be expected. Second, the validated measurement tools for study outcomes varied even among studies that examined the same health condition. Third, not all yoga interventions were described in detail in terms of poses, intensity and duration of each pose, and how breaths and meditations (when used) were incorporated into the sequence to allow for comparisons and replication. These methodological limitations and differences made reviewing these studies challenging.
Because yoga is considered to be a mind-body therapy that brings both psychological and physical aspects into harmony to improve health and a sense of wellbeing,32 a number of reviewed studies measured the effects of yoga on psychological effects and QOL. Eight of the 13 reviewed studies measured mental disorders (depression and anxiety), wellbeing, and/or health-related QOL. However, findings are inconsistent. Only three17,24,27 of the 8 studies reported significant improvement in mental health and/or QOL among participants in the yoga intervention, while 9 of 10 studies reported improvement in physical function or pain level. More RCTs, rather than a simple pre-test/post-test design, should be conducted to measure psychological effects, as a long-term effect of yoga intervention, with validated instruments at multiple points in time for accurate assessment.
A wide range of dropout rates were reported in the studies reviewed (0%-29%). Studies with positive results tend to be from those that had low dropout rates. Researchers from two studies that found yoga intervention did not have any significant effects suggested that such findings could be attributed to the low attendance rate at yoga classes and poor adherence to home practice.23,28 In order to evaluate yoga’s true treatment effects, it is important to assess barriers to participation. Future research should incorporate strategies that enhance yoga participation and adherence.
Practice Implications
Evidence regarding the effectiveness of yoga interventions for older patients with chronic health conditions has major implications for geriatric healthcare providers. Although there are limited data on the clinical applications of yoga among older patients, the preliminary results from this literature review suggest that it may be an important adjunct to treatment and should be considered in certain chronic health conditions. Healthcare providers may use a holistic approach in treating a chronic condition that is considered complementary to conventional medical treatments. If yoga can be used in conjunction with medication and other conventional treatments, older patients with chronic health conditions, who often are interested in seeking complementary therapies, may better manage their conditions. Based on a database of evidence of the effects of appropriate yoga programs on a variety of chronic health conditions (eg, Hatha yoga program for post-stroke patients), geriatrics healthcare providers will be able to encourage patients to include yoga in comprehensive treatment of their condition.14
Research Implications
Further large-scale controlled trials using rigorous methodology and reporting is needed to determine the efficacy and safety of yoga in older adults with chronic health conditions. Additional research on different chronic health conditions and studies that include a longer follow-up period (eg, 6 months, 1 year) are warranted to evaluate the therapeutic and long-term effects of yoga.
Strengths and Limitations
A major strength of this review is that it is the first critical review of the evidence on the safety and efficacy of yoga for managing chronic health conditions in older adults. This review included studies with high quality trial design published in peer-reviewed journals as well as in gray literature to minimize the chance of publication bias. The search used a large number of databases from multiple disciplines to reduce the risk of selection bias. However, heterogeneity of the included studies, limited number of studies focusing on the same chronic health condition, and a wide variety of yoga interventions and outcome measures precluded meta-analysis. Furthermore, the total number of trials included in this review and the total sample size are too small to allow definitive conclusions. In addition, this review included only community-dwelling older adults with chronic conditions; thus, the results may not be applicable to older patients in long-term care settings.
Conclusions
Despite yoga’s widespread popularity, scientific evidence that supported the use of yoga as a therapeutic intervention has not yet been established. While the studies reviewed were positive and supportive of using yoga for improving physical and psychological symptoms associated with a variety of chronic health conditions in older adults, the limited evidence available and methodological limitations preclude definitive conclusions on its effects and safety. More high quality research with larger sample sizes, well specified yoga interventions and sound methodology are needed to provide sufficient level of evidence to document yoga’s benefit in different chronic health conditions.
References
- Yoga definition. National Center of Complementary and Alternative Medicine website. http://nccam.nih.gov/health/yoga. Accessed October 30, 2013.
- Field T. Yoga clinical research review. Complement Ther Clin Pract. 2011;17(1):1-8.
- McCall T. Yoga as Medicine: The Yogic Prescription for Health and Healing. New York, NY: Bantam Dell; 2007:7-9.
- Healthy aging: helping people to live long and productive lives and enjoy a good quality of life, at a Glance, 2011. Centers for Disease Control and Prevention website. www.cdc.gov/chronicdisease/resources/publications/aag/aging.htm. Accessed October 30, 2013.
- Lee PG, Cigolle C, Blaum C. The co-occurrence of chronic diseases and geriatric syndromes: the health and retirement study. J Am Geriatr Soc. 2009;57(3):511-516.
- Exercise comes of age as medicine for older adults. President’s Council on Fitness, Sports & Nutrition. 2010;10(3):1-13. www.presidentschallenge.org/informed/digest/docs/june2010digest.pdf. Accessed November 1, 2013.
- Kooperman S, Ackerman L. Yoga for the 50+. American Senior Fitness Association website. www.seniorfitness.net/YOGA.htm. 2005. Accessed October 30, 2013.
- Cramer H, Lauche R, Haller H, Dobos G. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29(5):450-460.
- Cabral P, Meyer H, Ames D. Effectiveness of yoga therapy as a complementary treatment for major psychiatric disorders: a meta-analysis. Prim Care Companion CNS Disord. 2011;13(4).
- Aljasir B, Bryson M, Al-shehri B. Yoga practice for the management of type II diabetes mellitus in adults: a systematic review. Evid Based Complement Alternat Med. 2010;7(4):399-408.
- Lin KY, Hu YT, Chang KJ, Lin HF, Tsauo JY. Effects of yoga on psychological health, quality of life, and physical health of patients with cancer: a meta-analysis. Evid Based Complement Alternat Med. 2011;2011:659876.
- Macy D. Yoga in America. Yoga Journal. Published February 26, 2008. www.yogajournal.com/press/press_release/40. Accessed June 3, 2014.
- Chen KM, Tseng WS, Ting LF. Development and evaluation of a yoga exercise programme for older adults. J Adv Nurs. 2007;57(4):432-441.
- McCaffrey R, Park, J. The Benefits of Yoga for Musculoskeletal Disorders: A Systematic Review of the Literature. Journal of Yoga and Physical Therapy. 2012;2(5):1-11. www.omicsonline.org/the-benefits-of-yoga-for-musculoskeletal-disorders-a-systematic-review-of-the-literature-2157-7595.1000122.php?aid=8472. Accessed Nov. 1, 2013.
- Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1-12.
- Olivo SA, Macedo LG, Gadotti IC, Fuentes J, Stanton T, Magee DJ. Scales to assess the quality of randomized controlled trials: a systematic review. Phys. Ther. 2008;88(2):156-175.
- Ebnezar J, Nagarathna R, Yogitha B, Nagendra HR. Effects of an integrated approach of hatha yoga therapy on functional disability, pain, and flexibility in osteoarthritis of the knee joint: a randomized controlled study. J Altern Complement Med. 2012;18(5):463-472.
- Ebnezar J, Nagarathna R, Bali Y, Nagendra HR. Effects of an integrated approach of yoga therapy on quality of life in osteoarthritis of the knee joint: a randomized control study. Int J Yoga. 2011;4(2):55-63.
- Greendale GA, Huang MH, Karlamangla AS, Seeger L, Crawford S. Yoga decreases kyphosis in senior women and men with adult-onset hyperkyphosis: results of a randomized control trial. J Am Geriatr Soc. 2009;57(9):1569-1579.
- Donesky-Cuenco D, Nguyen HQ, Paul S, Carrieri-Kohlman V. Yoga therapy decreases dyspnea-related distress and improves functional performance in people with chronic obstructive pulmonary disease: a pilot study. J Altern Complement Med. 2009;15(3):225-234.
- Schmid AA, Van Puymbroeck M, Altenburger PA, et al. Poststroke balance improves with yoga: a pilot study. Stroke. 2012;43(9):2402-2407.
- Littman AJ, Bertram LC, Ceballos R, et al. A. Randomized controlled pilot trial of yoga in overweight and obese breast cancer survivors: effects on quality of life and anthropometric measures. Support Care Cancer. 2012;20(2):267-277.
- Vaishali K, Kumar KV, Adhikari P, UnniKrishnan B. Effects of yoga-based program on glycosylated hemoglobin level serum lipid profile in community dwelling elderly subjects with chronic type 2 diabetes mellitus—a randomized controlled trial. Physical & Occupational Therapy in Geriatrics. 2012;30(1):22-30.
- Manjunath NK, Tellers S. Influence of yoga and Ayurveda on self-rated sleep in geriatric population. Indian J Med Res. 2005;121(5):683-690.
- Chan W, Immink MA, Hillier S. Yoga and exercise for symptoms of depression and anxiety in people with poststroke disability: a randomized, controlled pilot trial. Altern Ther Health Med. 2012;18(3):34-43.
- Gordon LA, Morrison EY, McGrowder DA, et al. Effect of exercise therapy on lipid profile and oxidative stress indicators in patients with type 2 diabetes. BMC Complement Altern Med. 2008;8:21.
- Shahidi M, Mojtahed A, Modabbernia A, et al. Laughter yoga versus group exercise program in elderly depressed woman: a randomized controlled trial. Int J Geriatr Psychiatry. 2011;26(3):322-327.
- Chen KM, Fan JT, Wang HH, Wu SJ, Li CH, Lin HS. Silver Yoga exercises improved physical fitness of transitional frail elders. Nurs Res. 2010;59(5):364-370.
- Tüzün S, Aktaş I, Akarirmak Ŭ, Siphani S, Tüzün F. Yoga might be an alternative training for the quality of life and balance in postmenopausal osteoporosis. Eur J Phys Rehabil Med. 2010;46(1):69-72.
- Skoro-Kondza L, Tai SS, Gadelrab R, Drincevic D, Greenhalgh T. Community based yoga classes for type 2 diabetes: an exploratory randomised controlled trial. BMC Health Serv Res. 2009;9:33.
- American Thoracic Society. ATS Statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111-117.
- Pilkington K, Kirkwood G, Rampes H, Richardson J. Yoga for depression: the research evidence. J Affect Disord.2005;89(1-3):13-24.
Disclosures:
The authors report no relevant financial relationships.
Corjena Cheung, PhD, RN1; Juyoung Park, PhD2 ; Jean F. Wyman, PhD, RN1
Affiliations:
1School of Nursing, University of Minnesota, Minneapolis, MN
2School of Social Work, Florida Atlantic University, Boca Raton, FL