
Interactive Quiz: Abdominal Pain

Welcome to Consultant360's latest interactive diagnostic quiz. Over the next few pages, we'll present a case and ask you to make the diagnosis and treat the patient. Along the way, we'll provide details about the case, and at the end, we'll share the patient's outcome.
Ready to get started? >>
First, let’s meet the patient.
A 35-year-old man presented with moderate to severe, constant right-sided abdominal pain. The pain had been progressively worsening over the past 2 days and was associated with 1 watery bowel movement and nausea without vomiting. The pain was relieved with marijuana use and was not associated with food intake. Findings of a review of systems were otherwise negative.
His medical history was significant for Ehlers-Danlos syndrome (EDS) of unknown subtype and for intermittent tendinitis. His mother had systemic lupus erythematosus and autoimmune hepatitis, and his father also has EDS.
His vital signs were normal. Cardiac and pulmonary examination findings also were normal. Abdominal examination revealed tenderness over the right upper and lower abdomen, with normal bowel sounds and no masses. Examination of the extremities revealed hypermobility of the fingers, talipes equinovarus, and knee hyperextensibility greater than 10°.
Laboratory test results included the following values: white blood cell count, 14,500/µL; hemoglobin, 15.9 g/dL; platelet count, 207 × 103/µL; sodium, 135 mEq/L; potassium, 4.1 mEq/L; blood urea nitrogen, 14 mg/dL; and creatinine, 0.82 mg/dL.
Are You Correct? >>
Answer: A, Perform CT scans and echocardiography
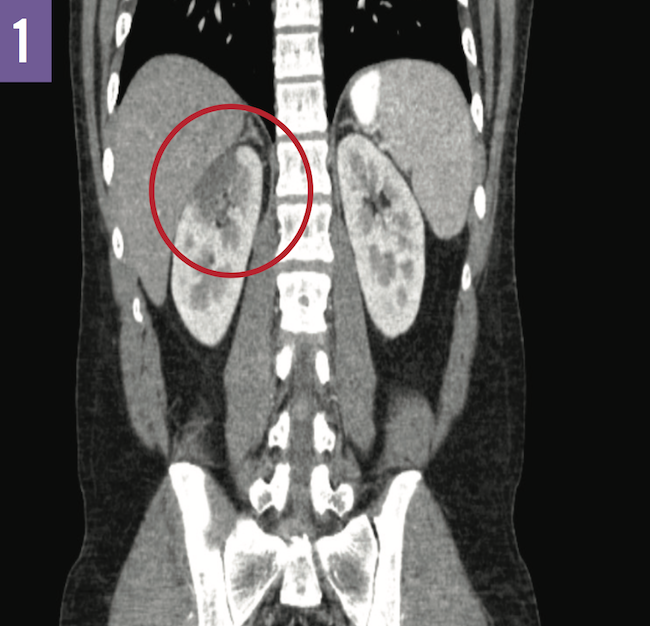
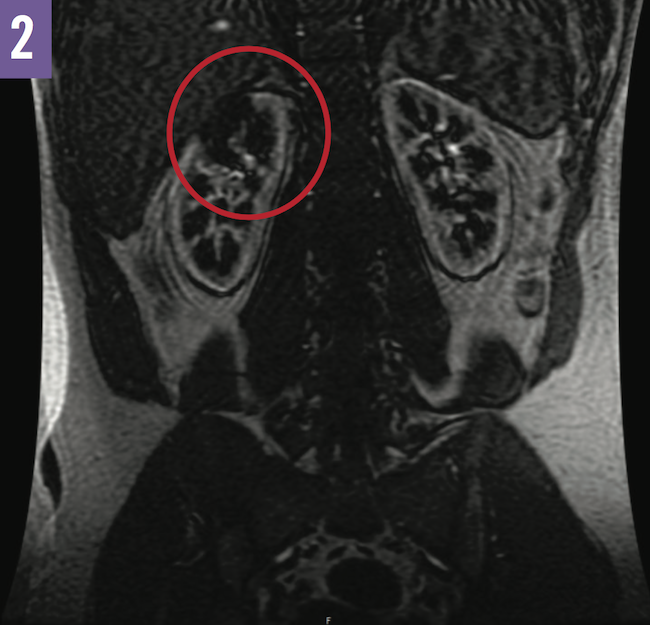
A number of imaging studies were done during his hospital stay. Computed tomography scans of the abdomen and pelvis were suggestive of a renal infarct as opposed to pyelonephritis (Figure 1). Transthoracic and transesophageal echocardiography revealed no apparent thrombi. Magnetic resonance angiography of the abdomen showed evidence of renal upper pole avascularization without abnormalities of the renal arteries (Figure 2).
Are You Correct? >>
Answer: B, Hypercoagulability workup
Results of a hypercoagulability workup and other tests were negative for factor V Leiden mutation, positive for hepatitis B surface antibodies, negative for lupus anticoagulants, and negative for prothrombin gene mutation.
The patient did have findings suggestive of EDS that could be diagnosed clinically as the classic type. However, the presentation of renal infarction raised concern for vascular type EDS, which is associated with significantly higher morbidity and mortality rates.
Are You Correct? >>
Answer: A, Lifelong anticoagulation therapy
Genetic medicine and vascular surgery teams were consulted, and it was decided that, irrespective of emboli or dissection, the patient should be placed on lifelong anticoagulation therapy.
The patient was then discharged home on long-term anticoagulation with warfarin and a goal international normalized ratio of 2 to 3.
Thank you for taking our interactive quiz! For more quizzes, visit the Resource Center.
This interactive quiz is based on:
Maanit K, Balaji Y. Renal infarction in Ehlers-Danlos syndrome. Consultant. 2017;57(12):718-719.
https://www.consultant360.com/articles/renal-infarction-ehlers-danlos-syndrome.