
Peer Reviewed
Sudden Respiratory Distress in Infants With Cardiac and Gastrointestinal Malformations
Authors:
Aman Chauhan, MD; Christopher Arcement, MD; Kelly K. Gajewski, MD; and Christian Lilje, MD
Citation:
Chauhan A, Arcement C, Gajewski KK, Lilje C. Sudden respiratory distress in infants with cardiac and gastrointestinal malformations. Consultant for Pediatricians. 2016;15(12);583-585.
Patient 1
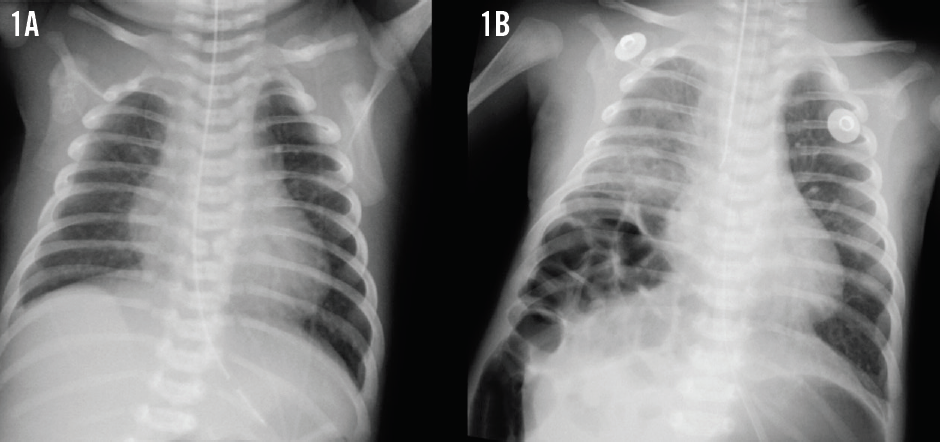
A newborn boy with a variant of unrepaired Tetralogy of Fallot had been sent for surgery for associated tracheoesophageal fistula, esophageal atresia, imperforate anus, and scrotal fistula. He also had asplenia and vertebral anomalies, but his chromosomes were normal. Postoperatively, he experienced persistent but asymptomatic gaseous bowel distension. During a routine cardiology clinic visit at 1 month of age, he developed respiratory distress unrelated to his heart defect. Pulse oximetry readings were 60% to 65% in room air, and breath sounds were diminished in the right lower quadrant. The infant was hemodynamically stable, and his pulmonary stenosis murmur was unchanged. A chest radiograph obtained 1 hour prior to the visit revealed mild cardiomegaly with increased pulmonary vascularity but no acute pulmonary disease (Figure 1A). The boy required ventilator support within hours. A repeat chest radiograph was obtained (Figure 1B).
Patient 2
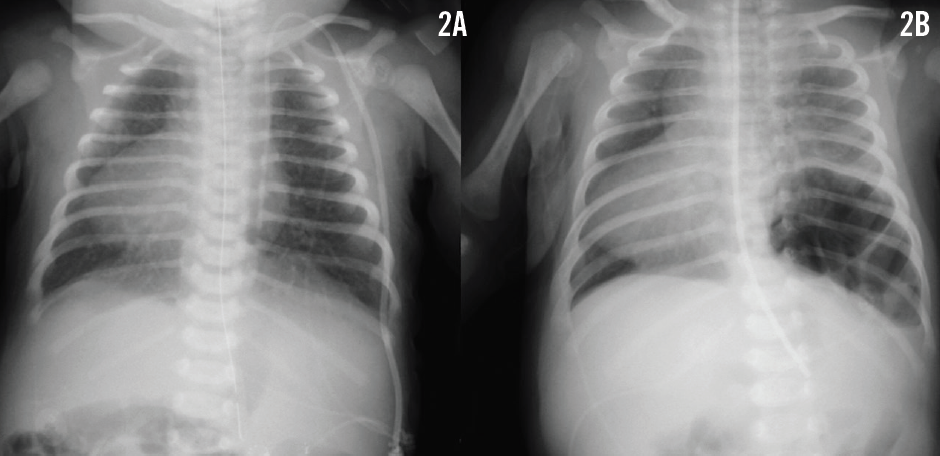
A newborn girl with complex cyanotic congenital heart disease and multiple extracardiac congenital anomalies, including heterotaxy with malrotation, had been sent for a Ladd procedure. Subsequently, the cleft palate was closed. She was also known to have asplenia yet had normal chromosomes. Her heart disease comprised dextrocardia with situs ambiguous viscero-abdominalis and situs inversus thoracalis, a primum atrial septal defect, tricuspid atresia, ventricular inversion, hypoplastic right ventricle, ventricular septal defect, malposed great vessels, and pulmonary stenosis. The results of a chest radiograph at 3 days of age confirmed the dextrocardia and revealed normal lungs (Figure 2A). At 5 weeks of age and long off ventilator support, the girl suddenly developed mild dyspnea. Breath sounds were decreased on the left, pulse oximetry readings were around 80%, and hemodynamic data were stable. A follow-up chest radiograph was obtained (Figure 2B).

What could be causing these symptoms in these 2 patients? >>
Answer: Delayed congenital diaphragmatic hernia
The results of the repeat chest radiograph in the first patient showed a right-sided posterolateral delayed congenital diaphragmatic hernia that was repaired the next morning (Figure 1B). Three months later, the patient again required emergent surgery for a perforated Meckel diverticulum. At 9 month of age, he underwent uneventful Tetralogy of Fallot repair.
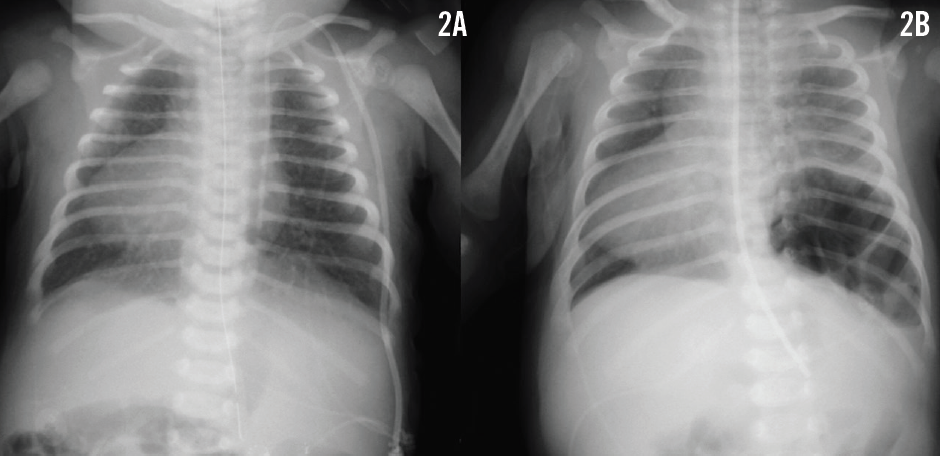
The results of the follow-up chest radiograph in patient 2 revealed a left-sided posterolateral delayed congenital diaphragmatic hernia (Figure 2B). The hernia was repaired along with a Nissen fundoplication procedure and a gastrostomy-tube placement. The patient subsequently required additional surgeries for gastrocutaneous fistula, pneumoperitoneum, and peritonitis. At 6 months of age, a left-sided bidirectional Glenn anastomosis was placed uneventfully. At 3 years of age, the Fontan circulation was completed. Both patients are now 5 years of age and are doing well.
DISCUSSION
These 2 cases of nonsyndromic delayed congenital diaphragmatic hernia have striking similarities. The delayed herniation was a sudden onset one-time event, well documented by previously normal chest radiographs. There was no pulmonary hypoplasia. Compared with a mean reported age at diagnosis of 372 days, the herniation in our 2 patients occurred relatively early.1 There was no evidence of infection, trauma, or iatrogenic lesions, which have all been suggested as triggering factors. Temporary defect occlusion by solid organs also appeared unlikely, as there was a midline liver in the patient with the right-sided hernia, and asplenia in the patient with the left-sided hernia. Both patients did surprisingly well from a cardiac standpoint despite having complex heart disease, but both experienced significant gastrointestinal morbidity.
Congenital diaphragmatic hernia is the result of incomplete fusion of the pleuroperitoneal folds.2,3 The prevalence is 2.4/10,000 births,2 and the vast majority (> 98%) are posterolateral hernias.3 Associated cardiac and gastrointestinal malformations, such as malrotation, have been observed in up to 45% and 16% of patients, respectively.2-7 Most patients present immediately postnatally in severe respiratory distress secondary to pulmonary hypoplasia. Morbidity and mortality are high, and 1-year survival is low.1,4,5,7
In contrast, delayed congenital diaphragmatic hernia—presenting beyond 31 days of age—is approximately 100 times less frequently encountered,1 and associated cardiac defects are about 3 times less common than in presentations that occur immediately postnatally.2,3,6 However, associated gastrointestinal malformations are about 3 times more common in delayed than in immediate postnatal presentations,5,7 and morbidity due to these associated defects is potentially considerable, especially in the case of abdominal surgical procedures.8
Overall mortality for delayed congenital diaphragmatic hernia is reportedly low if the patient is treated in a timely manner,4 but the correct diagnosis is easily missed.1 Thus, it is important for clinicians to be aware that a normal presymptomatic chest radiograph may be deceiving and does not exclude the diagnosis.5,6
The etiology of delayed congenital diaphragmatic hernia is not entirely understood. Factors such as traumatic or iatrogenic events, temporary occlusions of a preexisting defect by solid organs or prolapsing viscera, and group B streptococcal sepsis have been linked to the presentation. A pressure imbalance between the supra- and sub-diaphragmatic compartments has also been suggested as a causative element.1,3,5,7-10 Increased intraabdominal pressure was a likely scenario in our patients, but pulmonary hypoplasia is not considered a key factor. Fetal pulmonary development should be unaffected in delayed herniation.
On the other hand, pulmonary hypoplasia has been reported in up to 20% of patients, suggesting diagnostic uncertainty.7 It is unknown how many patients present with delayed symptoms rather than late-onset herniation. Normal presymptomatic chest radiographs have been documented in very few cases.6 Absence of pulmonary hypoplasia and/or documented absence of herniation prior to presentation may better define delayed congenital diaphragmatic hernia than the somewhat random age at presentation.1
Aman Chauhan, MD; Kelly K. Gajewski, MD; and Christian Lilje, MD, are from the Department of Pediatric (Cardiology) at Louisiana State University Health Sciences Center and Children’s Hospital in New Orleans, Louisiana.
Christopher Arcement, MD, is from the Department of Radiology at Louisiana State University Health Sciences Center and Children’s Hospital in New Orleans, Louisiana.
REFERENCES
- Kitano Y, Lally KP, Lally PA; Congenital Diaphragmatic Hernia Study Group. Late-presenting congenital diaphragmatic hernia. J Pediatr Surg. 2005;40(12):1839-1843.
- Dott MM, Wong LY, Rasmussen SA. Population-based study of congenital diaphragmatic hernia: risk factors and survival in Metropolitan Atlanta, 1968-1999. Birth Defects Res A Clin Mol Teratol. 2003;67(4):261-267.
- Robert E, Källén B, Harris J. The epidemiology of diaphragmatic hernia. Eur J Epidemiol. 1997;13(6):665-673.
- Colvin J, Bower C, Dickinson JE, Sokol J. Outcomes of congenital diaphragmatic hernia: a population-based study in Western Australia. Pediatrics. 2005;116(3):e356-e363.
- Heaton ND, Adam G, Howard ER. The late presentation of postero-lateral congenital diaphragmatic hernias. Postgrad Med J. 1992;68(800):445-448.
- Numanoglu A, Steiner Z, Millar A, Cywes S. Delayed presentation of congenital diaphragmatic hernia. S Afr J Surg. 1997;35(2):74-76.
- Hosgor M, Karaca I, Karkiner A, et al. Associated malformations in delayed presentation of congenital diaphragmatic hernia. J Pediatr Surg. 2004;39(7):1073-1076.
- Marhuenda C, Guillén G, Sanchez B, Urbistondo A, Barceló C. Endoscopic repair of late-presenting Morgagni and Bochdalek hernia in children: case report and review of the literature. J Laparoendosc Adv Surg Tech A. 2009;19(1):S95-S101.
- Gheibi S, Mahmoodzadeh A. Delayed presentation of right-sided diaphragmatic hernia after mechanical ventilation in a newborn with hyaline membrane disease: a case report. Med J Islamic Acad Sci. 2001;14(1):21-24.
- Rescorla FJ, Yoder Mc, West KW, Grosfeld JL. Delayed presentation of right-sided diaphragmatic hernia and group B streptococcal sepsis: two case reports and review of the literature. Arch Surg. 1989;124(9):1083-1086.