
Peer Reviewed
Myopathy in the Setting of Colchicine and Statin Coadministration
Authors:
Kartik Kalra, MD; Nabil Ghani, MD; and Kavya Patel, MD
Saint Peter’s University Hospital, New Brunswick, New Jersey
Citation:
Kalra K, Ghani N, Patel K. Myopathy in the setting of colchicine and statin coadministration [published online August 2, 2018]. Neurology Consultant.
A 61-year-old woman with a history of coronary artery disease, chronic kidney disease, gout, and hypertension (controlled with atorvastatin) presented to the emergency department (ED) with a chief concern of heaviness in both legs for 2 days. She reported that the leg heaviness had gradually worsened to the extent that she needed help getting out of bed and even walking on a flat surface. She also reported that 8 days prior to presentation, she had begun having pain and a burning sensation in her right foot. At that time, her primary care provider had initiated treatment with colchicine for a gout flare.
Physical examination. Upon arrival in the ED, the patient’s vital signs were normal. Neurologic examination revealed general muscle weakness and decreased sensation of the lower extremities. Bilateral symmetric hyporeflexia was present.
Diagnostic tests. Initial laboratory test results included a white blood cell count of 3100/µL (reference range, 4000-11,000/µL), a hemoglobin level of 10.5 g/dL (reference range, 13.0-17.0 g/dL), and a platelet count of 140 × 103/µL (reference range, 150-400 × 103/µL). The blood urea nitrogen level was 39 mg/dL (reference range, 6-20 mg/dL), serum creatinine was 1.89 mg/dL (reference range, 0.66-1.25 mg/dL), and serum potassium was 4.3 mEq/L (reference range, 3.5-5.1 mEq/L). Urinalysis demonstrated deep brown, turbid urine with a large amount of blood with 0-2 red blood cells per high-power field. The creatinine kinase (CK) level was 8579 U/L with a CK–MB fraction of 8.9 ng/mL (reference range, 0.6-6.3 ng/mL), and the lactate dehydrogenase level was 5542 U/L.
It was suspected that the patient was experiencing a drug-induced neuromyopathy, and colchicine and atorvastatin were discontinued. On day 2, electromyography results showed polyphasic motor unit action potentials with low amplitude and short duration, indicative of myopathy, with no evidence of demyelinating polyneuropathy to suggest Guillain-Barré syndrome.
Muscle biopsy results showed vacuolar myopathy with multiple small vacuoles in the center of the muscle fiber (Figure 1). Electron microscopy of a biopsy specimen showed lysosomes filled with autophagic material (Figure 2). These observations were consistent with colchicine toxicity. No signs of statin-induced myopathy, such as myonecrosis, were seen. After the discontinuation of colchicine, a rapid decrease of the CK level and recovery of the pancytopenia occurred. The muscle weakness disappeared gradually over 2 weeks.
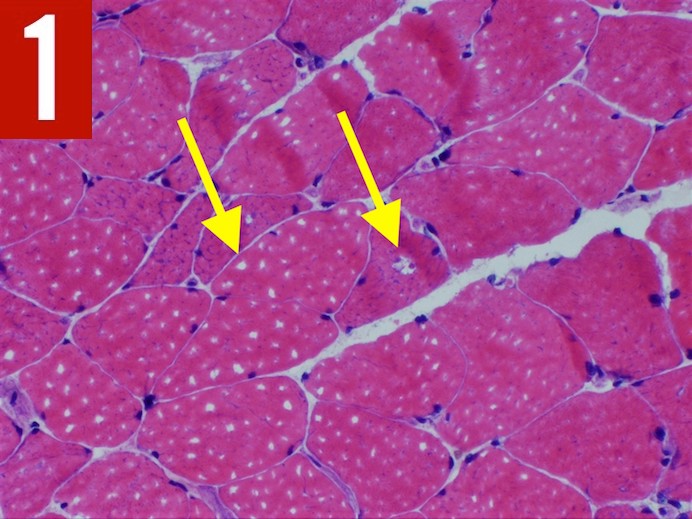
Figure 1. Muscle biopsy results showed vacuolar myopathy with multiple small vacuoles in the center of the muscle fiber (arrows).
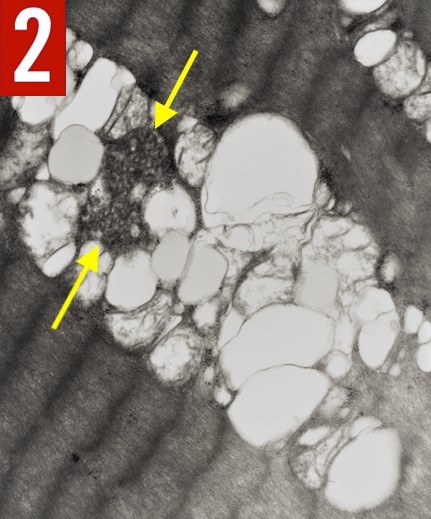
Figure 2. Electron microscopy of a biopsy specimen showed lysosomes filled with autophagic material (arrows).
Discussion. Although the microtubule polymerization inhibitor colchicine has been used for centuries, its neuromuscular toxicity in humans is largely unrecognized.1 In patients with chronic kidney failure, coadministration of colchicine and atorvastatin may accelerate the onset of myopathy, because the CYP 3A4 isoform of cytochrome P450 is crucial in the breakdown of both drugs.2
When adding colchicine to a medication regimen that includes a statin for patients with renal insufficiency, drugs that are metabolized outside the CYP 3A4 system (eg, fluvastatin, pravastatin) should be selected instead.3
Colchicine myopathy usually presents with proximal weakness and always presents with an elevation of the serum CK level; both features remit within 2 to 4 weeks after the drug is discontinued.4
References
- Wilbur K, Makowsky M. Colchicine myotoxicity: case reports and literature review. Pharmacotherapy. 2004;24(12):1784-1792.
- Rosenson RS. Current overview of statin-induced myopathy. Am J Med. 2004;116(6):408-416.
- Hsu W-C, Chen W-H, Chang M-T, Chiu H-C. Colchicine-induced acute myopathy in a patient with concomitant use of simvastatin. Clin Neuropharmacol. 2002;25(5):266-268.
- Molad Y. Update on colchicine and its mechanism of action. Curr Rheumatol Rep. 2002;4(3):252-256.