
Sexual Dysfunction in Older Men
Key words: Sexual dysfunction, androgen deficiency, male andropause, testosterone replacement therapy, phosphodiesterase-5 inhibitors, penile vacuum pumps, penile prostheses, self-injection therapy.
__________________________________________________________________________________________________
Physicians now understand that many older men retain an interest in sexual activity as they age. Some primary care physicians think that sexual potency in older males is normal, and that if it is lacking, it is “all in the head.” This viewpoint has not been supported by the literature. In one study from Massachusetts, nearly 50% of men older than 40 years reported having some form of sexual dysfunction.1 The myths that surround the problems of impotence, or erectile dysfunction (ED), confound the attempts of patients to receive treatment and the attempts of physicians to help them.
Many factors can contribute to sexual dysfunction in older men, including physical and psychological conditions, comorbidities, and the medications used to treat them. Aspects of an aging man’s lifestyle, his behavior, and the presence of an androgen deficiency (most often decreasing testosterone levels) may affect sexual function as well. A study of men between the ages of 30 and 79 years showed that 24% had testosterone levels below 300 ng/dL and 5.6% had symptomatic androgen deficiency.2
It has been reported that the percentage of men who engage in some form of sexual activity decreases from 73% for those aged 57 to 64 years to 26% for those aged 75 to 85 years.3 For some men this constitutes a problem, but for others it does not. A study by Lindau and colleagues3 that examined sexuality in older Americans showed that 50% of the men in a probability sample of more than 3000 US adults reported at least one bothersome sexual problem and 33% had at least two such problems.3 This article will review the normal changes that occur with aging, factors that influence these changes, individual variations and perspectives, and the available treatment options for ED and androgen deficiency.
Overview of Physiologic Changes and Risk Factors
As men age, they may experience changes in overall health and hormone levels. Such changes include decreased testosterone levels, decreased sperm count, increased difficulty in achieving erections, decreased strength of erections, decreased libido, and decreased force and volume of ejaculation. These changes may affect a man’s sex life and his ability to engage in sexual intimacy with his partner.
Male sexual dysfunction is often considered synonymous with ED, which is characterized by the inability to achieve a full erection or the inability to maintain an erection. The insecurity associated with ED can negatively affect a man’s confidence and lead to avoidance of sexual activity. Other types of sexual dysfunction, such as premature ejaculation and low libido, may occur; however, the most common and disruptive problem in men is ED. Although most men will experience periodic episodes of ED, these episodes tend to become more frequent with advancing age. The problem of ED, especially in older men, should not be ignored because it could be an outward sign of more serious diseases, including coronary artery disease, hypercholesterolemia, or diabetes mellitus.
Medical conditions, such as hypertension, diabetes mellitus, and cardiovascular disease, and psychological conditions, such as depression and anxiety, also contribute to sexual dysfunction in middle-aged or elderly men. Cardiovascular diseases and hypertension cause a narrowing and hardening of the arteries, leading to reduced blood flow to the corporal bodies, which is essential for achieving an erection. Diabetes is another contributor to sexual dysfunction because it can affect both the blood vessels and the nerves that supply the penis. Men with diabetes are three times more likely to experience ED, and they typically experience it 15 years earlier than men without diabetes.4 Obesity has also been correlated to the development of several types of dysfunction, including a decrease in sex drive and an increase in episodes of ED.4 Obese men often have low self-esteem, which further compounds these problems.
Medications used to treat some conditions often include ED or decreased libido as a side effect. Examples include hydrochlorothiazides and beta-blocking agents. Medications used to treat depression may also contribute to ED. Selective serotonin reuptake inhibitors are most commonly associated with ED. Such agents include citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline. In contrast, bupropion, which has a predominant effect on blocking the reuptake of dopamine, is an antidepressant associated with a lower incidence of ED.
Major health problems may not only weaken a man physically, but also shift his attention away from sex. Diseases—notably prostate cancer and its therapy—can be a direct cause of ED. Similarly, the illness of a man’s partner may interfere with the sex life of the couple. Finally, the loss of a partner and the unavailability of or unwillingness to find a new partner can negatively affect a man’s sex life. According to Lindau and colleagues,3 aging men are particularly vulnerable to the loss of a partner; close to 25% of all men aged 75 to 85 years in their study reported having neither a spouse nor an intimate relationship.
Role of Testosterone
Testosterone peaks in the late teens, then steadily declines with age, most noticeably for men older than 50 years. Having a low level of testosterone may cause a variety of symptoms, including fatigue, decreased libido, irritability, and depression, but the exact mechanism of action is not well understood and is an ongoing topic of study. Because the symptoms that accompany decreased testosterone levels in men are similar to those that accompany decreased estrogen levels in women during menopause, the terms andropause or male menopause have been used. Testosterone is known to play a main role in both sex drive and in the ability of a man to achieve erections.
A reduction in libido is widely considered the most prominent symptomatic reflection of low testosterone levels in men,5 and correction via supplementation therapy is regarded as a promising treatment for the symptoms of androgen deficiency, including reduced libido. Libido and testosterone concentrations are strongly related at the population level; however, the value of individual patient reports of reduced libido as indicators of low testosterone levels is open to question.5 The specific range of testosterone values that is associated with symptoms of sexual dysfunction may differ by patient, and response to supplementation varies with dose, age, and endogenous testosterone levels.6
A large endocrine screening program conducted in the late 1990s showed that 9% of men with ED who were older than 50 years met the diagnostic criteria for hypogonadism. During the First International Consultation on Erectile Dysfunction, the World Health Organization recommended that testosterone be assayed in men with low sexual desire and atrophic testes (≤19 mL), because ED secondary to hypogonadism is potentially reversible using testosterone replacement therapy,7 which is outlined later in this article.
Sexual Dysfunction Treatment Options
The good news is that there are many treatments available for men who struggle with sexual dysfunction, and they are not limited to the phosphodiesterase-5 (PDE-5) inhibitors. Increased exercise and physical fitness is negatively correlated to ED, whereas smoking, obesity, and watching television are directly correlated to ED.8 Changing these types of behaviors may be the most tangible way to improve sexual health as well as overall health. Making an effort to lose weight, exercise more frequently, cease smoking, and decrease alcohol consumption will improve sex drive and function for many men.
PDE-5 Inhibitors
When lifestyle changes are not enough to correct sexual dysfunction, drug therapy may be useful. The most common treatment for ED is a PDE-5 inhibitor taken 45 minutes prior to intercourse. This is referred to as on-demand use. Tadalafil is also available as a 5-mg daily dose, which may be more convenient for couples that find planning their sexual life around taking a pill unromantic.
The effect these agents have on an older man’s sex life depends on the etiology of the sexual dysfunction. For some men, these drugs can be an excellent solution. For men who have decreased sex drive or other health problems, however, they may have no effect. If a man with ED responds poorly to PDE-5 inhibitors, his serum testosterone level should be measured before considering the treatment a failure. If his testosterone level is decreased, adding testosterone replacement to the PDE-5 inhibitor will often restore his sexual ability. These responsive men typically have a combination of androgen deficiency and a possibly vasculogenic cause of ED. As a result, both testosterone and PDE-5 inhibitors are needed to successfully resolve the ED.
All men taking PDE-5 inhibitors need counseling on their proper use, as these agents alone do not cause erections; adequate genital stimulation is required. Sexual stimulation is vital because PDE-5 inhibitors potentiate nitric-oxide–mediated vasodilation only in the presence of sufficient sexual arousal. Patients should also be counseled to try using a PDE-5 inhibitor several times before declaring it ineffective; the cumulative probability of success with sildenafil, for example, increases with 9 to 10 attempts, after which it stabilizes.9
Men should take into account how taking such drugs will change the sexual relationship for their partners as well and make an effort to discuss it. Couples that have had a void in sexual intimacy for several years may have dual problems with sexual function. For example, an older female partner is likely to have estrogen deficiency and may also have an atrophic vagina and a contracted vaginal opening, which causes pain or discomfort during intercourse. If her partner starts taking PDE-5 inhibitors without her knowledge or understanding, she may not welcome the return of her partner’s virility. Men and their female partners should be counseled so that the woman has time to prepare both psychologically and physically.
Hormone Replacement Therapy
Hormone replacement therapy is an emerging treatment option for male andropause, and most often comprises testosterone replacement therapy. Testosterone can be self-administered as a gel daily or as an injection every 2 weeks. Alternatively, testosterone patches and buccal bioadhesive testosterone tablets can be used. More recently, testosterone pellets have become available, which can be inserted under the skin and replaced every 4 to 6 months. Most men will feel some improvement in energy, in sex drive, and sometimes in ED, although the degree of improvement depends on the individual. For example, treatment with medications that affect testosterone production or metabolism, such as glucocorticoids and opioids, may affect the response to testosterone replacement therapy.
Psychotherapy
Sexual dysfunction often has some psychological elements, whether depression, performance anxiety, or stress, that can be treated in conjunction with the underlying physical causes. Psychotherapy used with PDE-5 inhibitors has been shown to improve ED more successfully than use of this medication or psychotherapy alone.15
Vacuum Pumps
Vacuum pumps for treating ED involve creating a vacuum around the penis that forces blood into the corporal bodies. This blood is maintained within the corporal bodies by securing a ring around the base of the penis, enabling the penis to remain erect. Vacuum erection devices are usually tolerated and effective, with low morbidity and few recognized complications. A 2005 study showed that men who had moderate ED had a higher success rate with vacuum erection devices than patients with mild or severe ED.16
Research into the efficacy of and satisfaction with vacuum therapy alone has shown variable results, with patient satisfaction ranging from around 60% to as high as 82%,17 and little research has been done on the newer devices. Although many studies have shown good outcomes for achieving erections, they have also shown dissatisfaction with some aspects of the device, such as pain and the inability to achieve adequate erection for intercourse.18 Men, especially those older than 60 years, who used combined pharmacologic therapy with vacuum erection devices were more satisfied than those who used either therapy alone.19
Penile Prostheses
For those who have found little success with medications or other types of therapies, there are several surgical options. The most common is the insertion of an inflatable penile prosthesis. This is an elective procedure usually done under general anesthesia. The prosthesis is composed of a reservoir, a pump, and two tubes that mimic the corpora cavernosa. The pump is placed in the scrotum, where it can be accessed to self-inflate the tubes and create an erection. For men who were able to achieve orgasm before the surgery, orgasm will often still be achievable. Postoperative complications include infection and erosion, although these occur infrequently, at 5% and 8%, respectively.20,21
Most patients choose a penile prosthesis implant as a last resort when other therapies fail. With rates of efficacy in the ability to have intercourse of 89% and satisfaction rates of 81%, this can be a good option for some patients.20 Specifically, the inflatable penile prosthesis showed the highest rates of patient satisfaction, with scores of 81 on the Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS) questionnaire at 12-month follow-up.21 EDITS scores range from 0 (extremely low treatment satisfaction) to 100 (extremely high treatment satisfaction), with a score above 50 indicating treatment satisfaction.22
Counseling Regarding Risks of Sexual Activity and Therapy
Consensus guidelines have been issued for risk-stratifying and counseling patients with concomitant sexual dysfunction and cardiovascular disease.25 Men with both ED and cardiovascular disorders need to be informed that there is a transient increase in the relative risk of cardiovascular events during and within 2 hours after sexual intercourse. The absolute risk of having a myocardial infarction (MI) within each hour after sexual activity is considered to be low in otherwise healthy men with ED. Patients experiencing cardiac symptoms when initiating sexual activity should be counseled to seek medical attention immediately and to abstain from further sexual activity. An exercise echocardiography study by Pomara and colleagues26 showed that treatment with PDE-5 inhibitors did not adversely affect hemodynamic variables, exercise capacity (treadmill time), and/or time to cardiac ischemia (or first awareness of angina) in patients with stable coronary artery disease.
Sexual activity does have well-defined hemodynamic consequences, which can directly affect the heart. Studies have shown that heart rate, blood pressure, and respiratory rate can rise substantially during sexual activity, sometimes paralleling values seen with moderate exertion. All of these factors increase the amount of work the heart is required to do. Some men with underlying heart disease also experience angina during sex, a symptom that can warn of an impending MI. Standardized measurements of a person’s oxygen consumption, which demonstrate the degree of physical exertion the body is experiencing, have shown that at its peak, sexual activity is about as physically strenuous as walking 2 to 4 miles per hour.27 The greatest levels of exertion actually occur during orgasm, which lasts only briefly. People with a sedentary lifestyle, however, do seem to be at a mildly increased risk of having an MI after sex than their more active counterparts. This is congruent with well-established data that a regular exercise routine can reduce the risk of MI or sudden cardiac death related to physical exertion in general.28
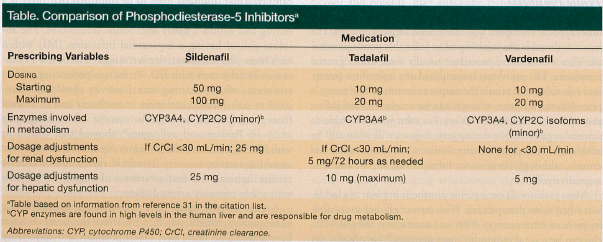
A rule of thumb regarding the prescribing of PDE-5 inhibitors is that men who can climb two flights of stairs without shortness of breath or chest pain are able to safely engage in sexual activity. The only absolute contraindication for using PDE-5 inhibitors is in a patient who uses any nitroglycerin formulation (eg, nitroglycerin, glyceryl trinitrate, isosorbide mononitrate). The use of nitroglycerin in conjunction with PDE-5 inhibitors may result in a precipitous decrease in blood pressure and a decrease in coronary artery blood flow. PDE-5 inhibitors are not contraindicated with the anesthetic agent nitrous oxide or with dietary sources of nitrates, including L-arginine, because neither contributes to plasma levels of nitric oxide.30 The Table compares the most commonly used PDE-5 inhibitors and the dosage adjustments needed for patients with renal or hepatic dysfunction.31
Evaluating Sexual Health
Healthcare providers should be aware of potential sexual problems in their aging male patients and aim to make them feel comfortable discussing these problems, enabling the provision of treatment and resources, if requested. It is equally important for providers to understand that a decreased interest in sex can be normal and acceptable to many aging men. In 2009, results of the National Social Life, Health, and Aging Project (NSHAP)32 showed that aging men have increasing rates of sexual dysfunction; however, it also showed other patterns of sexual behaviors and attitudes. For instance, it found that rates of masturbation declined with age, from 63.4% for men aged 57 to 64 years to 27.9% for men aged 75 to 85 years. The increased rate of ED between these two age cohorts is insufficient to explain this decrease. One possibility is that interest in sexual behaviors decreases with age. In fact, the NSHAP found that 25.9% of 75- to 8 5-year-old men surveyed also answered that sex was “not at all important” in their lives compared with 6.2% of 57- to 64-year-old men. Men in the 75- to 85-year-old cohort also showed an increase in unwillingness to have sex with a partner if they were not in love with that partner.32 In reality, declining interest in sexual activity, increasing rates of sexual dysfunction, decreasing hormone levels, decreasing availability of partners, and changing priorities and personal beliefs most likely all play some role in changes in sexual behavior of older men. All of these factors must be considered and weighed during discussions with patients.
Conclusion
ED and androgen deficiency are common conditions in aging men. The diagnosis is easily made during a history and physical examination, and a few blood tests, including serum testosterone level, can be useful. When a problem in sexual function is identified, therapeutic options are available for most men, and those options should be fully explored when men are troubled by sexual dysfunction. Finally, a thorough evaluation includes ascertaining individual attitudes regarding sexual activity and respect for the patient’s wishes regarding whether to pursue a specific therapy.
References
1. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinley JB. Impotence and its medical and psychological correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151(1):54-61.
2. Araujo AB, Esche GR, Kupelian V, et al. Prevalence of symptomatic androgen deficiency in men. J Clin Endocrinol Metab. 2007;92(11):4241-4247.
3. Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357(8):762-774.
4. Rosen RC, Wing R, Schneider S, Gendrano N 3rd. Epidemiology of erectile dysfunction: the role of medical comorbidities and lifestyle factors. Urol Clin North Am. 2005;32(4):403-417.
5. Travison TG, Morley JE, Araujo AB, O’Donnell AB, McKinlay JB. The relationship between libido and testosterone levels in aging men. J Clin Endocrinol Metab. 2006;91(7):2509-2513.
6. Gray PB, Singh AB, Woodhouse LJ, et al. Dose-dependent effects of testosterone on sexual function, mood, and visuospatial cognition in older men. J Clin Endocrinol Metab. 2005;90(7):3838-3846.
7. Bhasin S, Cunningham GR, Hayes FJ, et al; Task Force, Endocrine Society. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010;95(6):2536-2559.
8. Bacon CG, Mittleman MA, Kawachi I, Giovannucci E, Glasser DB, Rimm EB. Sexual function in men older than 50 years of age: results from the health professionals follow-up study. Ann Intern Med. 2003;139(3):161-168.
9. Carson CC. Erectile dysfunction in the 21st century: whom we can treat, whom we cannot treat and patient education. Int J Impot Res. 2002;14(suppl 1):S29-S34.
10. Marks LS, Mazer NA, Mostaghel E, et al. Effect of testosterone replacement therapy on prostate tissue in men with late-onset hypogonadism: a randomized controlled trial. JAMA. 2006;296(19):2351-2361.
11. Ramasamy R, Fisher ES, Schlegel PN. Testosterone replacement and prostate cancer. Indian J Urol. 2012;28(2):123-128.
12. Morgentaler A. Testosterone therapy for men at risk for or with history of prostate cancer. Curr Treat Options Oncol. 2006;7(5):363-369.
13. Moyer VA; US Preventive Services Task Force. Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157(2):120-134.
14. Carnegie C. Diagnosis of hypogonadism: clinical assessments and laboratory tests. Rev Urol. 2004;6(suppl 6):S3-S8.
15. Melnik T, Soares BG, Nasselo AG. Psychosocial interventions for erectile dysfunction. Cochrane Database Syst Rev. 2007;(3):CD004825.
16. Dutta TC, Eid JF. Vacuum constriction devices for erectile dysfunction: a long-term, prospective study of patients with mild, moderate, and severe dysfunction. Urology. 1999;54(5):891-893.
17. Baltaci S, Aydos K, Kosar A, Anafarta K. Treating erectile dysfunction with a vacuum tumescence device: a retrospective analysis of acceptance and satisfaction. Br J Urol. 1995;76(6):757-760.
18. Lewis RW, Witherington R. External vacuum therapy for erectile dysfunction: use and results. World J Urol. 1997;15(1):78-82.
19. Chen J, Sofer M, Kaver I, Matzkin H, Greenstein A. Concomitant use of sildenafil and a vacuum entrapment device for the treatment of erectile dysfunction. J Urol. 2004;171(1):292-295.
20. Minervini A, Ralph DJ, Pryor JP. Outcome of penile prosthesis implantation for treating erectile dysfunction: experience with 504 procedures. BJU Int. 2006;97(1):129-133.
21. Mulhall JP, Ahmed A, Branch J, Parker M. Serial assessment of efficacy and satisfaction profiles following penile prosthesis surgery. J Urol. 2003;169(4):1429-1433.
22. Lewis R, Bennett CJ, Borkon WD, et al. Patient and partner satisfaction with Viagra (sildenafil citrate) treatment as determined by the Erectile Dysfunction Inventory of Treatment Satisfaction Questionnaire. Urology. 2001;57(5):960-965.
23. Simmons M, Montague DK. Penile prosthesis implantation: past, present and future. Int J Impot Res. 2008;20(5):437-444.
24. Natali A, Olianas R, Fisch M. Penile implantation in Europe: successes and complications with 253 implants in Italy and Germany. J Sex Med. 2008;5(6):1503-1512.
25. NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA. 1993;270(1):83-90.
26. Pomara G, Morelli G, Pomara S, et al. Cardiovascular parameter changes in patients with erectile dysfunction using pde-5 inhibitors: a study with sildenafil and vardenafil. J Androl. 2004;25(4):625-629.
27. Cheitlin MD. Sexual activity and cardiac risk. Am J Cardiol. 2005;96(12B):24M-28M.
28. Muller JE, Mittleman MA, Maclure M, Sherwood JB, Tofler GH. Triggering myocardial infarction by sexual activity. Low absolute risk and prevention by regular physical exertion. Determinants of Myocardial Infarction Onset Study Investigators. JAMA. 1996;275(18):1405-1409.
29. Schwarz ER, Rodriguez J. Sex and the heart. Int J Impot Res. 2005;17(suppl 1):S4-S6.
30. Kloner RA, Mitchell M, Emmick JT. Cardiovascular effects of tadalafil. Am J Cardiol. 2003;92(9A):37M-46M.
31. Hemerson P, Cantrell MA, Wald M, Braasch MR. Erectile dysfunction: beyond the phosphodiesterase inhibitors. US Pharm. 2008;33(8):33-46.
32. Waite LJ, Laumann EO, Das A, Schumm LP. Sexuality: measures of partnerships, practices, attitudes, and problems in the National Social Life, Health, and Aging Study. J Gerontol B Psychol Sci Soc Sci. 2009;64(suppl 1):i56-i66.
Disclosures:
The authors report no relevant financial relationships.
Address correspondence to:
Neil Baum, MD
3525 Prytania Street, Suite 614
New Orleans, LA 70115