
Radiologic Abnormalities and Anomalies

Ventricular Aneurysm
Ventricular aneurysm is characterized by extreme thinning of the cardiac wall and a convex deformity of the external surface. This aneurysm is frequently associated with transmural infarctions, and it involves the anterior or apical area in 80% of patients. A chest film may disclose a bulge on the lower left ventricular contour, and calcium is commonly noted within the aneurysm wall.
Major complications of this condition include congestive heart failure, ventricular tachycardia, and arterial embolism. Rupture rarely occurs unless there is reinfarction at the site of the aneurysm. The prognosis is contingent on the size of the aneurysm, the function of the remaining myocardium, and the severity of coronary artery disease.
(Case and film courtesy of Drs Leslie Trope, William Bailey, and John DiTredici.)
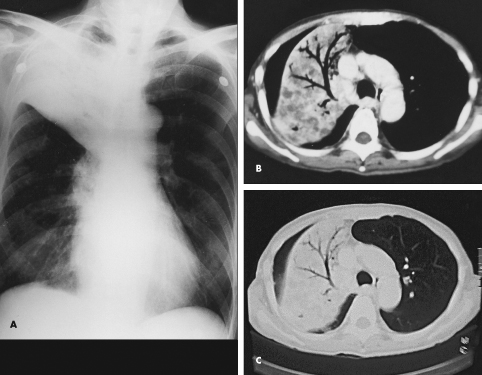
Hilum Overlay Sign in Anterior Mediastinal Tumor
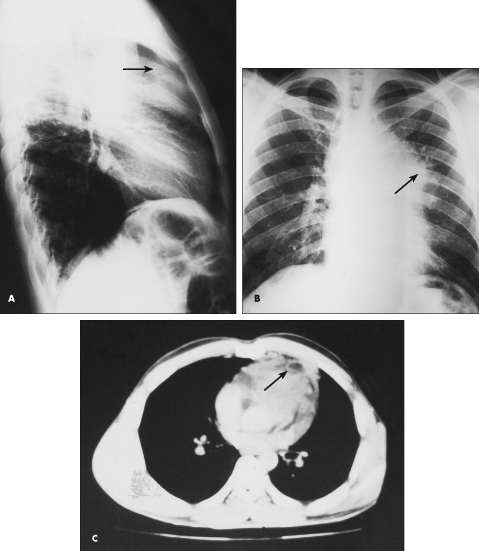
Fever of 1 month’s duration was this 28-year-old man’s only complaint. He had smoked marijuana in the past but denied intravenous drug use. His temperature was 39.4°C (103°F), but no other abnormalities were noted on physical examination.
A lateral chest film showed an anterior mediastinal tumor (A, ar-row). A posteroanterior film demonstrated the hilum overlay sign (B, arrow), in which the configuration of the anterior mediastinal tumor simulates an enlarged heart; the lungs appeared normal. Contrast-enhanced CT of the chest revealed mediastinal lymphadenopathy (C, arrow) with foci of necrosis.
Results of all laboratory investigations were negative. These included an HIV antibody test, a tuberculin skin test with 5 tuberculin units of purified protein derivative, and an examination of induced sputum smears and cultures for acid-fast bacilli. A CT-guided needle biopsy revealed a poorly differentiated large cell carcinoma.
Despite extensive diagnostic evaluation, the source of a primary tumor could not be identified. The patient responded well to combined radiation and chemotherapy, and his condition was stabilized within 6 months.
Surprisingly, an anterior mediastinal mass may closely resemble a dilated heart or pericardial effusion. The hilum overlay sign may be helpful in making this distinction. It is best shown on the anteroposterior Bucky film, in which the tumor is magnified more than the heart behind it, thus accentuating the discrepant position of the left pulmonary artery.
(Case, films, and scan courtesy of Dr Samer Alkhuja.)
Esophageal Foregut Cyst Presenting as Suprahilar Mass
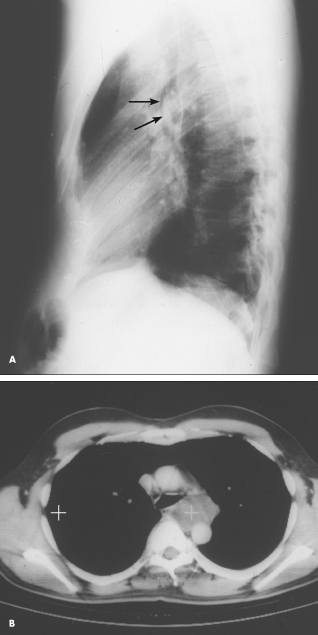
A chest roentgenogram from a 42-year-old man with asthma, primary hypoparathyroidism, and pectus excavatum showed a left suprahilar mass-like density (A, arrows). A CT scan showed this to be a cystic lesion to the left of the esophagus and posterior to the left main-stem bronchus (B, white cross). At surgery, it proved to be a 6.5 3 5.5 3 4-cm tense, tan, thin-walled unilocular esophageal foregut cyst, which was resected. The cyst contained a clear, mildly mucous fluid. The smooth inner cyst wall was approximately 1 mm thick and consisted of ciliated epithelium overlying connective tissue.
(Case, film, and scan courtesy of Drs Susan H. Allen and Terry Hoyt.)
Mediastinal Lipomatosis
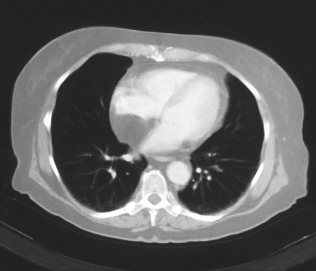
An obese 56-year-old woman was hospitalized after 2 days of chest pain, shortness of breath, and palpitations. Physical examination revealed no abnormalities, and serial cardiac enzyme studies and an ECG ruled out myocardial infarction. However, transesophageal echocardiography showed a lesion in the mediastinum.
A CT scan of the chest revealed a mass in the mediastinum, and the diagnosis of mediastinal lipomatosis was confirmed by the tumor’s characteristic low density (from 220 H to 2100 H). The patient’s chest pain subsided without any intervention. Two years later, the mass showed no change in size, confirming a benign process.
Lipomatosis is often associated with obesity, corticosteroid treatment, or Cushing’s disease. In most cases, the lesions are benign, although liposarcomas do arise in the mediastinum.
(Case and scan courtesy of Drs Ashwani Bhardwaj and Pritam S. Badesha.)
Bronchoalveolar Carcinoma
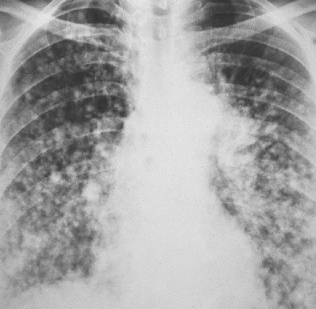
A 52-year-old woman (a nonsmoker) was hospitalized after experiencing a low-grade fever and dyspnea for a month. No abnormalities were noted on physical examination, but the chest film showed multiple nodules, both well- and ill-defined. Lung biopsy confirmed the diagnosis of bronchoalveolar carcinoma.
This neoplasm is considered a subtype of adenocarcinoma that arises from the terminal bronchioles and alveoli. It is seen predominantly in young women and is initially asymptomatic. The lesions are usually an incidental finding on a screening roentgenogram. Some patients have a history of cough, chest pain, increased dyspnea, low-grade fever, malaise, and weight loss.
(Case and film courtesy of Drs N. K. Akritidis, N. Georgogiannis, and C. Katsulidis.)
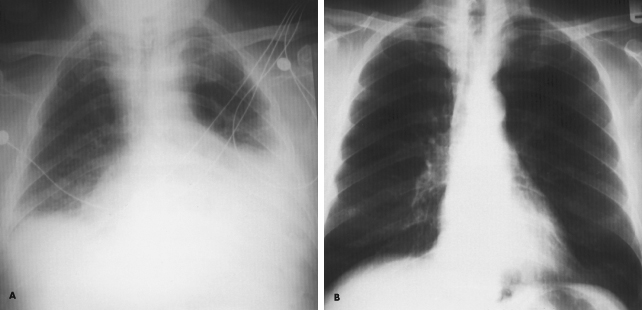
Myxedema Heart
Over the previous 6 months, a 59-year-old man had experienced lethargy, fatigue, poor appetite, cold intolerance, and abdominal distention. His vital signs were normal; physical examination revealed periorbital and pretibial edema, distant heart sounds, and delayed reflexes.
An ECG showed low voltages, and a chest film revealed generalized enlargement of the cardiac silhouette with a globular configuration and small, bilateral pleural effusions (A). An echocardiogram confirmed the presence of a large pericardial effusion. Subsequent laboratory studies revealed serum thyroid-stimulating hormone levels of 50 µU/mL, serum thyroxine levels of 4.5 µg/dL, and a reverse triiodothyronine uptake of 24.7 ng/dL. These findings are consistent with primary hypothyroidism. Thyroid replacement therapy was initiated. One year later, the chest film changes had resolved (B).
The recognition of pericardial effusions is important because these may, in a short time, lead to cardiac tamponade. Causes of such effusions include trauma, pericarditis, renal failure, Dressler’s syndrome, neoplastic disease, and immunologic disease (particularly rheumatoid arthritis and systemic lupus erythematosus). Pericardial effusion is a common finding in myxedema, occurring in up to one third of all cases.
(Case and films courtesy of Drs Eugene Wong and Peter Petropoulos.)
Air Bronchogram
For the past 3 months, a 66-year-old man has suffered fatigue and loss of appetite and weight. He was not coughing, nor had he experienced fever, chest pain, or hemoptysis. He had no history of notable respiratory disease, and he was not aware of having had tuberculosis (TB).
The patient had smoked a pack of cigarettes daily for 40 years but stopped smoking 6 years ago. He did not drink alcohol and had no risk factors for HIV infection.
Except for a temperature of 36.8°C (98.2°F) and signs of right upper lobe consolidation and possible collapse, physical examination results were unremarkable. Hyponatremia was the only laboratory test abnormality.
A chest film confirmed right upper lobe consolidation and also showed compensatory emphysema and elevation of the right hilum without tracheal shift (A). Because this was a marked collapse, the density of the lobe blends with that of the right superior mediastinum. CT of the chest revealed consolidation with partial collapse of the right upper lobe and an air bronchogram with cavitation or bronchiectasis (B and C). No masses were detected.
Examination of induced sputum showed acid-fast bacilli. Sputum cultures grew Mycobacterium tuberculosis. The patient was treated with four TB medications and showed good clinical and radiologic response.
Air bronchogram is usually associated with alveolar lesions, such as an inflammatory process, infarct, contusion, alveolar cell carcinoma, or lymphoma. Its presence without cavitation or bronchiectasis, however, may radiologically simulate pyogenic bacterial pneumonia. In this case, clinical data and further investigation should be applied to diagnose the underlying entity.
(Case, film, and scans courtesy of Dr Samer Alkhuja.)